QR codes are easy to produce, resistant to damage, and can hold a considerable amount of data. But generally speaking, eating them has no practical purpose. Unfortunately the human digestive tract lacks the ability to interpret barcodes, 2D or otherwise. But thanks to the University of Copenhagen, that may soon change.
 A new paper featured in the International Journal of Pharmaceutics details research being done to print QR codes with ink that contains medicine. The mixture of medicines in the ink can be tailored to each individual patient, and the QR code itself can contain information about who the drugs were mixed for. With a standard QR reader application on their smartphone, nurses and care givers can scan the medicine itself and know they are giving it to the right person; cutting down the risk of giving patients the wrong medication.
A new paper featured in the International Journal of Pharmaceutics details research being done to print QR codes with ink that contains medicine. The mixture of medicines in the ink can be tailored to each individual patient, and the QR code itself can contain information about who the drugs were mixed for. With a standard QR reader application on their smartphone, nurses and care givers can scan the medicine itself and know they are giving it to the right person; cutting down the risk of giving patients the wrong medication.
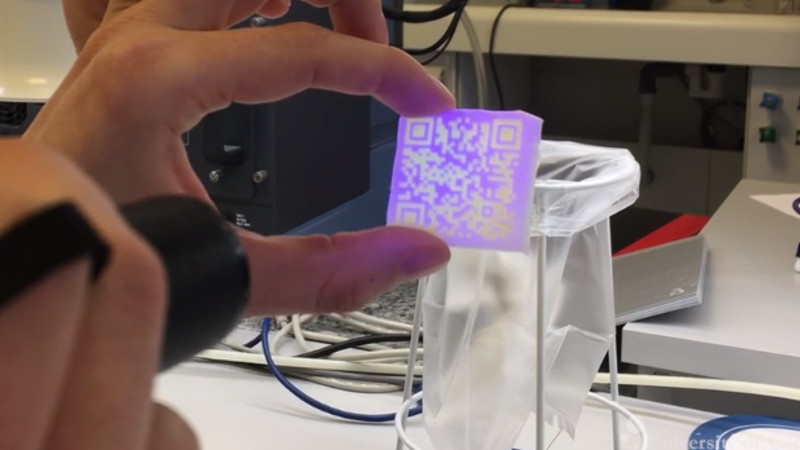
The process involves using a specialized inkjet printer to deposit the medicine-infused ink on a white edible substrate. In testing, the substrate held up to rough handling and harsh conditions while still keeping the QR code legible; an important test if this technology is to make the leap from research laboratory to real-world hospitals.
In the future the researchers hope the edible substrate can be produced and sent to medical centers, and that the medicinal ink itself will be printable on standard inkjet printers. If different medicines were loaded into the printer as different colors, it should even be possible to mix customized drug “cocktails” through software. Like many research projects it seems likely the real-world application of the technology won’t be as easy as the researchers hope, but it’s a fascinating take on the traditional method of dispersing medication.
QR codes have long been a favorite of the hacker community. From recovering data from partial codes to using them to tunnel TCP/IP, we’ve seen our fair share of QR hacks over the years.
[Thanks to Qes for the tip]












I guess you could design it to print the QR code and if you had the ability to selectively print specific ingredients in certain spaces and fill the rest with null spaces to finish the code, one could accomplish this sort of dual purpose printing plus drug effect.
Still, not sure I follow exactly what value it brings to society at large specifically unless the marginal cost and potential for problems were essentially zero.
Also unclear though how this would work in practice in terms of patient compliance or even basic understanding compared to the status quo. Dispense somebody a QR code drug and they are going to look at you rather quizzically.
Interesting idea but there are also some unintended issues, such as a greater surface area of the drug which could potentially lead to dosing irregularities, drug “wear” through handling, etc.
One value it brings to society would be a more reliable drug distribution among populations that are not particularly well organised, think of an old peoples home with too few caring staff for example. That medicine on a table next to some patients, it was prescribed for whom, when?
Yes, this is exactly the idea here.
I don’t understand why so many of the comments seem obtuse about why this could be extremely helpful in places where they have to distribute medications to many people. Perhaps they are just lucky enough that they’ve never seen the inside of such a facility, and don’t know how slipshod they can be.
I don’t know that it changes the problem. Conventional pills with the same QR code on the bottle label or cap provides much the same benefit, while the “printed medicine” approach requires those same slipshod nursing homes to be drug compounding facilities too, with all the rigmarole that entails, and IT people too to deal with the added technology dependency stack. Imagine the headlines when Grandma doesn’t get her medicine because the internet went down and couldn’t authorize the chipped cartridges, or the PC that runs the smart drug printer caught a ransomware, or the printer broke/clogged and there wasn’t a hot spare, or the same idiot who can’t keep the pill bottles straight didn’t order new ‘ink’ ahead of the expiration date, or…
Standard practices for hospitals (at least the one I work for) primarily work just like this.. a cart is used with a scanner that a nurse rolls into the patient’s room. They scan the bracelet of the patient and then the dispensed medicine (from pyxis which handles its labels) to confirm the patient/dosage is correct..
This could be great for places who don’t have these existing safe guards though!
maybe the comments are not obtuse but just considering the unintended consequences of adding complexity to an already bad situation. I have spent a fair ammount of time in hospitals and i understand how slipshod they could be which is why i question such an invention on the principal of adding complexity to the situation. It is one thing to sort pills and print labels for containers, but once you start printing the actual medicine you run into a whole host of issues.
first, cleaning such a printer and the general exposure of the printer to the hospital environment is going to drive the price up on the printer. This is due to either the printer will have to be completely sealed or will have a complex cleaning process which will require specialist training.
second, storage of the printable materials, solid drugs have a much longer shelf life than liquids and are less prone to contamination. This means that there will have to be more fridges on premises as well as the extra access procedures to get at such things.
Thirdly, profit, all of the above posturing eventually removes profit from the drug manufacturers as it will generally cost a whole lot more and thus eat into the margins of the drug producers as countries with the bargaining power are not going to pay the same rates if now they have to support extra machinery for drug delivery.
finally FMEA, Failure modes, the proposed methods seem to reduce the failure modes by moving the labeling and checking of drugs to a computer yet there are still humans in the loop and there will still be errors, especially since it relies on the humans using a device that was designed to take attention away from the task at hand (cellphones)
Its not a bad idea but it still needs several iterations before its ready to become a product
Except it does not bring this value in isolation. Now, instead of pills that are relatively easy to administer ad manufactured elsewhere with economies of scale, you now also have an entire critically important hardware and software stack to deal with. In addition, patients and staff alike may be unfamiliar with what is happening. Is every drug even physically suitable for this? Not all drugs share the same solubility profile and some are not even solids. Do these all need to be “printed”? How does viscosity or surface energy or evaporation profiles impact the printing or curing process? Does every drug even adhere to the surface? How about approval? Does moving it from pill form to something else change the relevant approval process?
I hear what you are saying but fail to see how this presents as a magical solution to suddenly, cheaply or easily solve or make more robust drug distribution and administration in otherwise poorly organized facilities.
yes, I agree, this just massively complicates things. How many medicines are in fairly common usage? Lets say about 100 (probably a low estimate). This means we have to have some kind of printer that has 100+ types of ink, and channels, how much is this going to cost? You are spot on with the physical properties of the different drugs presenting problems. Usually, things like the crystal structure of the drug can have a huge impact on its availability (does it dissolve in the stomach or does it just end up coming out the other end?). How much material can you get on one of these papers? Some drugs need doses of 500 mg or more.
“With a standard QR reader application on their smartphone, nurses and care givers can scan the medicine itself and know they are giving it to the right person; cutting down the risk of giving patients the wrong medication.”
Unlike a standard pill bottle with a QR code.
Or a bottle with a bar code. I’m sure this QR thing will catch on any day now. Technically superior, but so was Betamax.
If a nurse is holding a tray full of pill bottles she’s really not able to scan them and hand them out with the other hand.
And that how it often ends up being distributed. Medical care is a bulk thing.
And yeah you could build the scanner into the tray so you can just hold it at the edge to scan or something, but they won’t.
Medication can be in the wrong bottle. Having the QR code to verify directly on the medication what it is before the patient takes it can help prevent injury or death. It happens in the medical field.
Of course that assumes the QR code is printed correctly.
Don’t be silly, they couldn’t possibly cock that one up!
… or (radical idea I know) simply put the medication in a bottle with a human readable printed label… perhaps stating the dose, frequency and… maybe even the patients name… in actual writing.
That way the nurse doesn’t need a bloody smart phone just to try and figure out whether she is dispensing the correct random piece of blurry square blotch marked rice paper, or attempting to administer the stock code label that fell off the packet of bedpans.
This looks to me like a solution in need of a problem.
or a solution that will generate more problems?
I want to be the guy that gets the contract to sell hospitals all the smartphones which are just low end custom android smartphones. Chaching!
But then patient recognition goes down. “I usually have the blue pill, why is this one red?”.
That’s the whole point, once the pill comes out of the bottle you don’t know who it’s for anymore or in some cases what it even is.
Have you been to something like an assisted living facility? Somebody takes all the pills for each person and puts them into little paper cups and then another person distributes them. But what happens if somebody forgets which cup goes to which person?
With this method, not only could they potentially mix multiple medicines into one code (instead of taking 5 individual pills, say) there’s no way to confuse who it’s for as long as somebody is scanning it before handing it out.
Way too many potential failure points to make it better than the current system.
Printer breaks down. No drugs can be administered for the whole facility.
Wrong print cartridges used to cue up the drug cocktail.
Wrong patient entered into the system.
Wrong dispensing mix (printing drugs which interact).
Wrong patient dispensed to due to poor training on the complex system.
Wrong patient dispensed to due to two printed sheets sticking together.
Wrong dose due to due to poor training on the complex system.
Wrong medication dispensed due to inability to read the QR code due to equipment failure and assumption that correct medication has been issued.
Wrong (double, triple etc) dosage due to overprinting of the same information on the same sheet.
Wrong dosage due to poor print quality (this is an inkjet system… probably the least reliable printing method known to man).
Wrong drug administered due to poor cleaning of the machine.
etc. etc..
So rather than print the necessary information on the label itself in human-readable form, we’re putting a QR code in its place and scanning that with a barcode scanner to present similar information on a screen…?
Or, are humans meant to get good at reading QR codes by eye… like how they learned to read Morse code by ear?
And the statement “QR codes […] can hold a considerable amount of data” is bogus. With all the framing and required white space and error correction, you can convey the same information in human-readable dot matrix form using a quarter the number of ink dots. I’d wager it’s just as readable by a phone in this human-readable form too, these days.
While the statement “QR codes […] can hold a considerable amount of data” IS technically false, what they are getting at is that the reading smart phone isn’t limited to displaying JUST what is encoded in the QR code. The code could have nothing more than a patient ID number and a drug ID number, and the phone could display the patient’s picture and what the drug is being used to treat in this instance, which would make it far easier to tell if a mistake had been made.
I can’t be the only one thinking “personalized acid tab”
Just don’t make it in brown. I heard that’s bad. (oh, dear, am i *that* old already?)
Yeah I had that thought also, “Scan the tab for details about your next trip” LOL
That might be a generational thing.
Hmm. Built into the wristbands for a “Deadhead” reunion tour.
Heck, how practical would this be for those states with (pseudo)-legal edible cannabis products?
And it lets me also think of the quite low dose you could administer in this way (printed or droped on a paper like surface), a few 100µg. Something like penicillin or Aspirin is usually dosed at a level of several 100mg, up to 1g. You need a square meter of carrier substrate for that.
I was thinking the same thing. A good way to hide your cid! Not that I use it anymore!
Pointless. Just print the persons name and photograph for ID purposes. Simple, Easy, and much less error prone than a QR code.
Careful what you suggest, If the FDA gets ahold of an idea like that you could end up with a tri-fold pamphlet dose by the time they add the paper-cut on your tongue warnings ..
Umm… why not just put a tiny QR code on a regular pill? o_O?
or another code entirely…
Unless you’re talking some big horse pills, it would be too small.
Plus that’s not something you can do at the end point, they would have to be manufactured like that.
Give me a laser marking/engraving machine and you’ll see how they can be marked at the end point :P
I know pills printed with tiny letters, <1mm. The ink-jet dot matrix printer which does this can for sure also print a QR code.
This is as useless as it is pointless.
However on the plus side, it is as pointless as it is useless.
Oh.. but wait… I get it… vendor lock in… you need to buy our very expensive ink cartridge of generic drug, and use our pointless and buggy app to administer said drug.. DRM managed life saving medication…. Its the asprin equivalent of the Juicero.. lets call it the Drugero(tm) … now why didn’t you just say that… find enough mugs, and then come back to take my money…
https://www.youtube.com/watch?v=_Cp-BGQfpHQ
Cross contamination of drugs. You’d have to print a cleaning sheet after every ingredient change, and medications are expensive enough as they are without having to waste them cleaning nozzles.
The medications themselves aren’t generally that expensive, it’s more about the licensing cost that offsets the cost of development… and keeps the shareholders in caviar and yachts…
How about the QR code being printed, and having text to back up what the QR refers to (double check) and have a pick and place machine put the medications onto the tape with a sugar glue so the medicine directly beneath the QR and Text code is the medication meant to the patient? Allows for double verification, accuracy of pick and place (hell, even put a small printed copy of the markings of the medication ON the dispensed tape), and cuts back on Pharmaceutical distribution errors in places of high volume — Hospitals and large care facilities.
Pick and place pill popper… now that could be a thing.
Use real off the shelf drugs in real pill bottles.
Remember the pill is the drug delivery system, there is a reason why some are gell filled, others have microcapsules, others still use very specific binders to slow their release in the gut.
Getting rid of the pill is actually counterproductive.
Dispensing them in suitable trays automatically in large hospital pharmacies with a pick and place type arrangement however does seem like a more workable idea than re-inventing the entire drug delivery system to use “ink” and paper, just so you can turn the ink into an unnecessary QR code.
How true, I just forgot this also. You can’t print e.g. a time release capsule.
The QR code scans as Haloperidol for a made-up patient named Magnus Edinger. I feel bad that Magnus has either Schizsophrenia or Tourette Syndrome. They could have picked a more mild condition.
I licked my screen and the paper tasted like sugar, so it is probably a placebo.
Not a made up patient but one of the PhD students working on the project (named in the linked study), not sure if Magnus actually has that prescription though.
*sing*Lucy in the sky with diamonds…
Why a QR code?
Why not just human readable text? From the pictures it looks like it would fit. I’m pretty sure most nurses are busy enough as it is. They don’t need to stop, pull out a cellphone, open a QR app and screw around with getting just the right distance and angle for it to register. Just write the information that they need to know on the acid drop I mean medication so at a glance they know what they need to do and can just get on with it.
Not to mention, if they have a tray of these things, imagine scanning one then someone asks a question or walks around behind you… Now look back at the tray. That one, third from the left, that’s the one you scanned right? Sure it is, there isn’t time to scan it again. Give it to the patient already. Oh.. whoops!
Wonder about surface/storage characteristics – will it pick up germs, fungi, serve as growth medium.
Pills can be designed with a fairly impervious surface.
Will the substrate absorb water over time, will it mold, etc.
What drugs will survive the printing process (heating, etc.) unaltered.
What reactions happen between drugs or between drugs and ink?
(if printing multiple drugs together, they get much more chance to react with one another than
if in separate pills.)
Only good for “chewable” drugs (ones could be released in the mouth).
(Assume they don’t expect you to swallow that whole wafer.)
Not sure how many drugs can be done in chewable/disolve in mouth form – most seem to be swallow the pill form.
Most pharmacies moved away from compounding (which is what this would be), so this would require a reversal of that trend. (Greater oversight, responsibilities, etc.)
Looks like those QR codes my grandma ate at Woodstock.