2020 saw the world rocked by widespread turmoil, as a virulent new pathogen started claiming lives around the globe. The COVID-19 pandemic saw a rush on masks, air filtration systems, and hand sanitizer, as terrified populations sought to stave off the deadly virus by any means possible.
Despite the fresh attention given to indoor air quality and airborne disease transmission, there remains one technology that was largely overlooked. It’s the concept of upper-room UV sterilization—a remarkably simple way of tackling biological nastiness in the air.
Warm Glowing Killing Glow
Upper-room UV systems sound kind of like science-fiction technology. They nuke nasty pathogens in the air, and do it while emitting a faint and weird-colored glow. In reality, they’ve been quietly hanging around for about 80 years. The idea is straightforward enough—you just shine UV-C light in the unused overhead zone of a room to zap airborne pathogens before they get inhaled by fragile humans!
The concept came about as a direct result of 19th-century research that determined sunlight inhibited the growth of undesirable microbes and pathogens. Later work determined that light in the UV-C range of wavelengths is remarkably good at killing both bacteria and viruses, making it ideal for sterilizing purposes. The UV-C range is from 100 to 280 nanometers, but peak sterilizing action occurs around the 250-270 nm range. The primary method of action is that the UV-C light creates defects in DNA molecules that kill or inactivate microscopic organisms, including bacteria and viruses. It’s perfect for tackling all sorts of nasties, from measles to SARS to TB.
Unfortunately, that also means that UV-C light isn’t always safe to use around humans. Just as it hurts microbes, this light is also harmful to our skin and eyes in exactly the same way. Indeed, a prime example of this was a 2023 event that allegedly accidentally used UV sterilization lamps as decorative blacklights. While UV-C light is used in a wide range of sterilization applications, most keep the light hidden or localized to avoid direct human exposure.
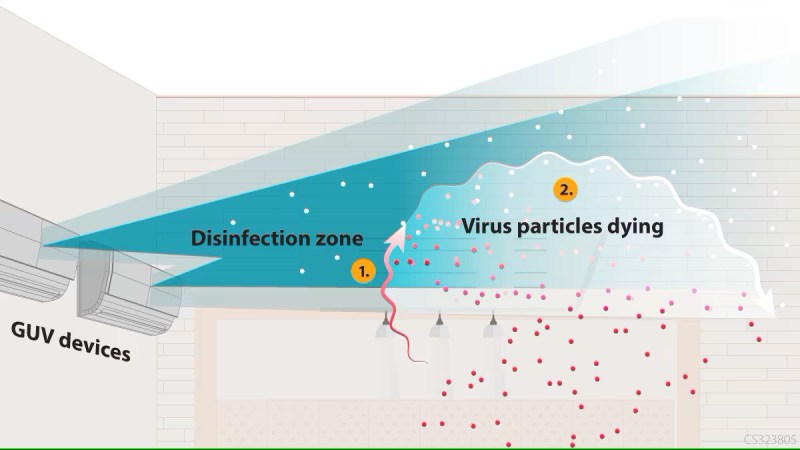
Upper-room UV-C installations are particularly interesting, though, for their simplicity. To avoid dangerous exposures, these installations simply place the sterilizing lamps up high in a room and direct their light into the upper level of air. As long as the UV light output is directed into the top level of the room, well above the heads of any occupants, it can sterilize the air effectively with little risk of harm.

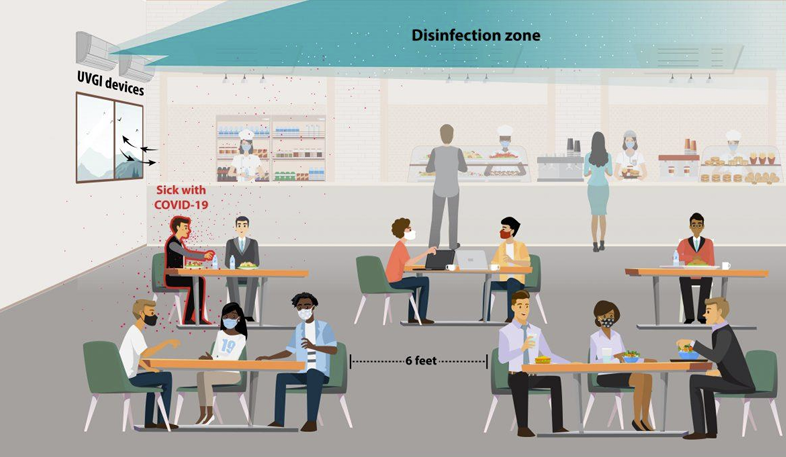
For this reason, these systems are typically installed in places like schools, hospitals and other public buildings, where ceiling heights are high enough to make such installations safe. CDC guidelines suggest minimum ceiling heights must be at least 8 feet for these installations, though 8.5 feet is preferred. For most people, that’s high enough not to cause trouble, but if you’re one of the taller players in the NBA, you might want to take note.
Upper-room UV systems treat a massive volume of air simply by sectioning the room into a germ-killing overhead zone and a safer lower zone where people breathe. Natural convection, HVAC currents, and even a simple ceiling fan help keep the air circulating upward, doused by the UV field, and then returned to the lower portion, scrubbed clean. At least a minimal level of circulation is required in order to ensure all the air in a given room is being treated. Power levels required are relatively low. A 2015 study suggested a total output of just 15-20 milliwatts is enough per cubic meter of room volume, assuming adequate air mixing in the space.
 Ultimately, though, proper sizing and safe installation are critical for creating an effective and safe sterilization system. UV-C is safe enough when used properly, but get it wrong, and you’ll see plenty of sore eyes and red skin almost immediately. The key is blocking direct and reflected UV light from reaching the lower zone of the room. Louvered fixtures with carefully aimed beams are necessary in rooms with lower ceilings, while more open fixtures are more for lofty spaces where they can blast UV upward without frying everyone’s eyeballs. Proper metering must be done at the time of installation to ensure light concentration is high enough in the sterilization region, and below safety limits in the occupied region. It’s also important to ensure the lamps are switched off for maintenance or if anyone is entering the upper zone of the room for any reason.
Ultimately, though, proper sizing and safe installation are critical for creating an effective and safe sterilization system. UV-C is safe enough when used properly, but get it wrong, and you’ll see plenty of sore eyes and red skin almost immediately. The key is blocking direct and reflected UV light from reaching the lower zone of the room. Louvered fixtures with carefully aimed beams are necessary in rooms with lower ceilings, while more open fixtures are more for lofty spaces where they can blast UV upward without frying everyone’s eyeballs. Proper metering must be done at the time of installation to ensure light concentration is high enough in the sterilization region, and below safety limits in the occupied region. It’s also important to ensure the lamps are switched off for maintenance or if anyone is entering the upper zone of the room for any reason.
It might sound high-tech, but this approach predates modern pandemics by decades. It was already showing its effectiveness against diseases like measles and tuberculosis as far back as the 1930s and 1940s. Early success was found at Duke University in 1936, where post-surgical infections were cut from 11.62% to just 0.24% with the use of an operating room eqiupped with UV-C equipment. Later, a 1941 study determined that UV-C delivered by mercury-vapor lamps had drastically reduced measles transmission in classrooms.

Given its efficacy, you might think that upper room UV-C installations would be everywhere. Subways, airports, schools, hospitals, and malls could all benefit from this technology. However, it would require some investment and ongoing maintenance, and it seems that simple cost is too much to bear.
For whatever reason, upper-room UV remains an obscure technology, seldom discussed and rarely used. Here we are, after countless deadly airborne disease outbreaks, still largely ignoring a century-old technology that actually works. The simplicity is staggering—slap a UV fixture on the wall near the ceiling, tune it so that zero harmful light hits the occupants, and let it run. It’s not a silver bullet for all air quality concerns, and you still need ventilation, of course. But for dealing with nasty airborne pathogens? It’s hard to imagine an easier solution than upper-room UV. The only real question left is, why aren’t we using it everywhere?
Featured image by the US CDC.













Paint the ceiling with fluorescent dyes, and you get twice the bang for the buck with illumination.
doesn’t work like that for uv-c
How do you think normal florescent bulbs work?
“No, we won’t be filling this workspace with all day long with low-level UV spill because light never reflects or diffuses, right?. Besides, what could possibly go wrong, after all, it’s not like UV light exposure is very strongly correlated with developing cataracts or anything”
Light follows the “inverse square law,” so every time the distance from the source doubles, the intensity is a quarter. If the source and the first reflective area is large enough, only a tiny fraction will reach the surface.
And the surface will never be 100% reflective, because a large part of the incident radiation will be absorbed, and part will be reflected away from the occupants of the room. The inverse square law is applied again, this time over a very weak light.
I doubt a well designed UVGI installation would increase the UV exposure enough to cause any detectable health effect. And when in doubt, there are commercial UV measuring devices that can tell exact how much UV is on the environment, and the installation can be tuned if the exposure is above limits.
*if the distance between the source and the first reflective are…
True, but if you’re working in an office or retail space with extra UV, “over time” means 2000 hours a year.
Depending on the hazard, exposure time can be as significant as exposure intensity.
If you’re cutting the intensity of the noise from a loud machine by a factor of 100 you might go from being able to be around the source for a few minutes without causing damage to being around it indefinitely.
But if you’re working around a reasonably tolerable level of, say, dioxin or radiation, prolonged exposure still adds up and sooner or later you start growing tentacles in inconvenient places.
If you’re working 2000 hours a year then you need to rethink your life choices 😂
That’s 50 weeks times 40 hours.
That’s a bare minimum work week with weekends off and two weeks vacation.
And, really, ‘rethink your life choices’? So what’s a person to do that is in that situation, ‘rethinks their life choices’ and then still has to spend several more years before they become fabulously wealthy and can live a life of leisure – like you do.
…until someone brings a Mylar helium balloon to the party.
The inverse square law only applies to isotropic sources.
Take a laser for example: the intensity is almost the same when you’re at twice the distance.
No. This is a popular misconception and incorrect. A laser behaves like any other light source. It absolutely follows the same inverse-square dropoff.
But, just like any other light source, if you are close to it (i.e., in the near field) and the beam is focused or collimated then the inverse square law does not apply, just like any other light source.
Ah yes, the very famous non-spatially-coherent laser. Very well known
The beam is ALWAYS affected in some way by a lens with common lasers, so this isn’t a convincing explanation. I’ll try and talk myself into a better one. (Take the lens off the front and it emits a narrow cone, or perhaps a fat line bounded by said cone. Even flashlights, headlights, etc almost never just put a flat domeless LED behind a window. They almost always have a reflector or a lens of some kind.)
The bit about near field sounds a little like circular reasoning without explaining the purpose of the definition. With lasers as I understand it, the term is defined as the portion of the beam before the focal point / beam waist. And that’s not going to immediately please anyone because it seems readily evident that you can focus a laser such that there is no waist. (If it is equal or very slightly less than collimated, as you’ve focused just slightly further away than infinity, the divergence is only very slightly more than the minimum possible). Maybe that can be resolved to a virtual source without the lens, idk.
That all being said, of course you can arrange things such that a divergence of millimeters beam radius per meter beam distance turns into a squared increase of beam area, reducing intensity to the constant power over the increased area. But it seems like it’s much more useful to see this by using the definitions and some logic to describe when something is and isn’t relevant. When the beam isn’t yet apparently diverging, it’s not got the inverse square as it’s not got the millimeters per meter. Since it’s not perfect, of course, to keep from diverging it’s going to be converging, and after that near field it’ll diverge eventually. But that can be at a fair distance, with many lasers. It’s kind of a point of them that you can use them inside a certain distance without that.
With a laser or a parabolic antenna, the physical emission source is not the same as the effective emission source, so even if the inverse square law still applies, it is strongly biased since it applies from the effective emission source. As a result its attenuation as seen from the physical source does not follow the inverse square law.
What you say is strictly correct, and true for any light source that incorporates any kind of lens or reflector to direct the beam. There’s nothing magical about laser light. Heck, every telephoto lens ever made does the same trick of moving the apparent source location to a location that’s different from from its actual physical location.
In practice, in any typical handheld or chip-scale laser the apparent source location is still going to be inside the laser. In particularly contrived demonstrations or special cases that employ a collimator and relatively large diameter beams operating in the near field, the apparent location can be some distance behind the physical light source body (whether or not it’s a laser!). And that’s true: it will bias the calculation, but the inverse square law still applies.
If you have any doubt, just measure it: Aim your favorite laser at a wall a few meters away, measure the diameter of the spot. Double the distance and measure again. What do you see?
For a real mindbender, you can even (fairly easily) construct an optical system in which the apparent source location is behind the observer (pericentric or hypercentric optics). It’s all in the optics, not the laser light.
The installation requires measurement of the UVC irradiance of the lower room with special attention to eye level to ensure that UVC exposure is at a safe level. It also recommends use of UVC absorbing pigments in paint such as titanium dioxide.
yeah the idea seems like a non-starter to me. constant exposure is a big deal, even at low levels. and you know the technicians installing these things are not going to do a good job of verifying there aren’t any hot spots in the habitable space. and probably less than 10% of installations will last a decade without substantial untested changes to the upper spaces. i have a hard time believing that mass deployment of these things will not result in some vision damage down the road
We manufacture and install this kind of lamps and the ceiling doesn’t reflect enough to be measureable if properly sized. We use very expensive spectrometers to make sure no light gets to where a human body part might be. UV-C reflects very differently than visible light, there aren’t many commonly used materials that do a good job reflecting those wavelengths. In devices we actually want to have a reflector behind the lamps we have to use polished aluminium because stainless doesn’t do a great job and glass mirrors reflect next to nothing (UV-C doesn’t go through normal glass or most clear plastics).
So what are typical installation costs (and in what part of the country, since obviously prices will vary with labor costs and such)? Are we talking only about institutional installations, or is it in a price bracket where a homeowner with high ceilings in at least one room could consider it?
“It’s also important to ensure the lamps are switched off for maintenance or if anyone is entering the upper zone of the room for any reason.”
This. Like when it’s time to change a (regular) ceiling-mounted light fixture.
Put the lamp in the ducts of forced air ventilation.
There it would minimize the destruction of surfaces caused by UV.
This, exactly.
And — bonus — you can even add a HEPA filter there while you’re at it, for when the UV lamp fails :-/
My home HVAC system has UVC lights in both the return air and distribution plenums. They are powered through the same safety interlock as the furnace itself.
These were installed about 20 years ago.
Yeah, but that costs money, giving minimum wage employees cataracts is free.
You would have to buy and install these devices into every room. Putting UV-C lights into an HVAC system is much much much cheaper.
Businesses love gadgets more than solutions.
There are very effective HVAC solutions as well. These include downdraft + floor returns and energetic filtration. These technologies should be mandatory in new building codes to help make civilization resistant to pandemics.
It’s all so tedious
Yeah, there’s a reason this isn’t common despite UV-C light sources being available for over 50 years. Firstly, the safety aspect makes this impractical in an open areas – reflections aren’t easy to “eliminate” unless one has complete control over the structures size and shape. And would have to ensure there are no protruding parts in the ceiling – you know like, light fittings, or fans, which would clearly reflect significant UV. I think people often underestimate the damage UVC can do to the eyes. And whilst “low-level” chronic exposure isn’t well studied, and obviously won’t be as bad as acute high level exposure, I’m going to say it probably isn’t great. Even if workers in the areas chronically exposed wear clothes that cover most of the skin – their face will be exposed at all times.
Secondly, air absorbs UVC so its range is limited. This is generally a positive since it limits exposure distance, but it also means large rooms may need emitters on opposite walls. It’s why UVC sterilisation is best done in enclosed spaces – air ducts, water pipes etc.. where flow can be controlled, and the UV can be fully contained.
Thirdly, it’s not like you can just wave a beam of UVC over a surface and its germ-free. It takes time, and only works where there are no shadows caused by uneven surfaces, for say, oblique exposure.
Honestly, doing this all in aircon would be easier, cheaper, less dangerous and arguably much more effective – which is exactly why it is used in this application.
Forgot to add: this only affects airbourne virus/fungal particles. It does nothing for the surfaces on the lower part of the room covered in droplets inevitably expelled by people talking, which is the more common route for many viruses. Had to add this in case we get folks suggesting this technology somehow reduces the need for basic sanitation – it doesn’t.
What about ozone production? my little lamp for pacifier disinfection produces ozone (I can tell from the smell)
“they also output some light in the visual spectrum that gives them a characteristic green glow” It is bluish or perhaps cyan to me, not green. Who is color-blind?
The recommendation is for use of low-pressure UVC lamps which do not generate ozone.
Maybe some don’t produce ozone. But the one the facilities chap put up at work stank of ozone. So we measured the air in the space and it was well above the UK limits for 15 minute exposure (0.2 ppm). Varied a bit around the room. From 8 ppm near the lamp to approaching the 0.2 ppm further away. Stank…
It is not permantly turned off :)
The short lifespan of the UV-C bulbs, high power usage, low efficiency (lots of heat per mW of UV-C), the damage done to many plastics, all work against the use of UV-C for this purpose. It is much easier, safer and cheaper to just install hepa filters and call it good.
Once UV-C LEDs become more efficient (around 20% last I knew) and cost effective, then this might be worth looking at again, but as others have pointed out, doing this in air ducts is the best method and still does nothing for non-airborne contaminants.
Good on paper, but of limited use (currently) in the real world.
I like the in-air-duct solutions for limiting ionizing radiation exposure to room occupants (although catching the burned out lamps could be a pain), but we could also periodically vacate rooms to do ozone treatments if we were actually concerned.
(We could also stop the CDC and WHO from taking junior high school science projects as gospel, but one thing at a time.)
back when the ronna was a big deal my work put in a hands free dryer in the bathroom that claimed all kinds of BS, at the end of the day it was a normal hand dryer with a UV LED that shines in your hands connected to a leaf blower that directs 10000CFM directly under the stalls kicking up god knows what in the air … good job
There is one in most Walmart’s and big entrances where people don’t hang out. I always thought it was to kill flies etc. I knew it was UV long before now.
I believe the fly lamps are UV-A, and use what’s essentially a blacklight bulb.
Seems like it needs to be paired with the narrowband filtered eximer lamp tech. I don’t trust this not to have some amount of reflections, and I also don’t trust eximer lamps to actually be 100% safe.
I did a bunch of reading on this topic. Many wavelengths of UV turn oxygen into ozone, and ozone is bad to breathe. This is why you shouldn’t use ionic blow dryers or ionic air filters. Some wavelengths of UV seem to actually reduce ozone, so they’re a better bet. But they do still create other kinds of ions, and it’s unclear how much health risk this creates. So the most conservative approach is to stick with HEPA filters. Next would be puraclenz or uvc in the ducts. Note that in a place like a hospital where you know there are pathogens, the ion/ozone risk may be worth it, and that’s where I’d contemplate overhead UVC.
Made me think of the requirements for having laser shows, and the tremendously strict requirements if you want to do something like a liquid sky effect where you scan a beam through fog overhead. The equipment has to have a key interlock, an operator, and physical blockers that prevent the beam from dipping down into the crowd.
I forget what the min height is, but they take into account people climbing up on each others’ shoulders.
Granted, exposure to UVC is a much slower eye-killer, but still I wonder.
I was thinking if they made UVC wavelength lasers it would be a good way to control the exposure. You could sweep horizontally with a galvo and have a strip of absorbing material to prevent reflection.
or a lens or shaped reflector to spread it into a line. galvo seems overkill for a fixed pattern, and adds danger (higher peak power if you do get swept by it). and i’d want that strip pretty wide, because who knows how securely the unit will be mounted, what happens as the walls shift and settle, etc. i’m definitely finding the arguments for existing in-duct applications compelling
UV lights? Germ theory?
Don’t worry, there are people trying to make this (254nm wavelength light) and FarUVC (222nm wavelength light) available to all: https://iuva.org/IUFUST-2025
here is the supporting research for the UV 222nm frequency for airborn viruses -this freq does not damage skin and corneas
https://www.nature.com/articles/s41598-022-08462-z
As a student I worked in a hospital, in the operating room. There were of course UV lamps placed high up, they were turned on when there was no one inside (I was in charge of their operation).
Now there is music played during operations. The patient is offered to choose the musical style (no hard-rock) but usually it is stopped as soon as he is anesthetized…
would cannibal corpse be acceptable? songs about getting your guts ripped open prior to having your guts ripped open seems oddly appropriate.
humans did not evolve to live in a germ free environment.
besides if the house is too clean the cats will mess it up to compensate.
Agree. That is what our immune system is for :) . Only need ultra-clean spaces for ‘specific’ cases. Work place isn’t one of them.
humans did not evolve to work in crowded rooms, therefore something which slows down the infection transmission could be useful.
With Covid the whole purpose of social distancing was to allow microscopic droplets expelled by other peope to fall downwards before hitting you square in the face, running fans to pull them up into the air could have negative consequences as they then have the potential to travel further… I guess it makes less difference if the virus is ordinarily airborne for longer as it is usually expressed. Just an observation.
The illustration is a hoot.
Social distancing and masking, neither of which were effective (because people wear masks improperly and usually inappropriate materials) alongside this method leads one to infer that this method will be just as effective;)
If it’s use became more wide spread, it would increase the likelihood that something would adapt to it.
I hear flouroantimonic acid makes an excellent mouthwash, too – it leaves absolutely no bacteria alive in what used to be an oral environment.
This tech is great and all, but UV-C is still light, and light diffuses and reflects – leading to inadvertent exposure. Not a good plan. A better application would be containment within an air processing unit, like the filter sump for a central air system.
My first thought (okay, my second thought) what is whether it would be worth adding UVC inside a Corsi-Rosenthal box, how much baffling would be required to do it safely, what the relative efficiency is of the two approaches and how they would combine if the filter is already stopping most pathogens.
Or perhaps reverse the flow on the CR box so UVC is being applied to the active surface of the filters, and use additional fans for room circulation.
My guess is this wouldn’t likely be effective. I suspect the amount of time the air would be exposed inside a CR box would be too brief. I’m pretty sure these UVC systems rely on a much slower air circulation rate to expose the viruses for a longer period of time to kill them.