
An interesting and also annoying aspect about the human immune system is that it is not a neat, centralized system where you input an antigen pattern in one spot and suddenly every T and B lymphocyte in the body knows how to target an intruder. Generally, immunity stays confined to specific areas, such as the vascular and lymph system, as well as the intestinal and mucosal (nasal) parts of the body.
The result of this is that specific types of vaccines have a different effect, as is demonstrated quite succinctly with the polio vaccines. The main difference between the oral polio vaccine (OPV) and inactivated vaccine (injected polio vaccine, or IPV) is that the former uses a weakened virus that induces strong immunity in the intestines, something that the latter does not. The effect of this is that while both protect the individual, it does not affect the fecal-oral infection route of the polio virus and thus the community spread.
The best outcome for a vaccine is when it both protects the individual, while also preventing further infections as part of so-called sterilizing immunity. This latter property is what makes the OPV vaccine so attractive, as it prevents community spread, while IPV is sufficient later on, as part of routine vaccinations. The decision to use a vaccine like the OPV versus the IPV is one of the ways doctors can tune a population’s protection against a disease.
This is where the current batch of commonly used SARS-CoV-2 vaccines are showing a major issue, as they do not provide significant immunity in the nasal passage’s mucosal tissues, even though this is where the virus initially infects a host, as well as where it replicates and infects others from. Here intranasal vaccines may achieve what OPV did for polio.
Going For The Gut Punch
Logically, targeting intranasal (IN) vaccines to address a coronavirus makes a lot of sense, since coronaviruses are among a group of viruses implicated in e.g. the common cold. Like rhino- and adenoviruses, they are viruses which are strongly adapted to the respiratory system, much like how the polio virus prefers the intestinal tract. Because of this knowledge, multiple intranasal vaccines have been developed and approved, most recently in India and China.
The Chinese vaccine is developed by CanSino Biologics, and it is essentially the same as the regular viral vector-based intramuscular (IM) vaccine, except in a form that allows it to be inhaled in a nebulizer. It is approved for use as a booster after a primary IM-based vaccination course.
The Indian vaccine (BBV154), produced by Bharat Biotech, is intended as a two-dose IN vaccination, rather than only as a booster. Both the CanSino and Bharat vaccines are based on a non-replicating adenovirus vector, which means that no special vaccine formulation is needed for the nebulized form. Upon inhalation of the nebulized vaccine, the adenovirus vector will simply do what it naturally does: get into mucosal cells to deposit its genetic payload.
These IN vaccines join the Iranian Razi Cov Pars vaccine (three-dose recombinant protein subunit-based with IN booster), which received emergency use authorization in Iran on October 31st of 2021. While large-scale efficacy data is not available yet for any of these vaccines, a recent US study in mice has confirmed that a viral vector-based vaccine can induce robust immunity. In a 2021 study by Van Doremalen et al. using the ChAdOx1 nCoV-19/AZD1222 (AstraZeneca) viral vector it was found that IN vaccination of hamsters and macaques prevented large-scale infection and significantly reduced the mucosal viral load.
These findings are essentially why scientists in the West are pushing for IN vaccines to be made available, with some US scientists, including Scripps Research’s Eric Topol, calling for an IN equivalent of the Operation Warp Speed (OWS) which originally produced the IM vaccines that have been in use in Europe and North America since late 2020. The hope is that an approved IN vaccine in the West may counteract the continued spread of the SARS-CoV-2 virus amidst waning efficacy of the IM vaccines against new virus variants.
The Long Haul
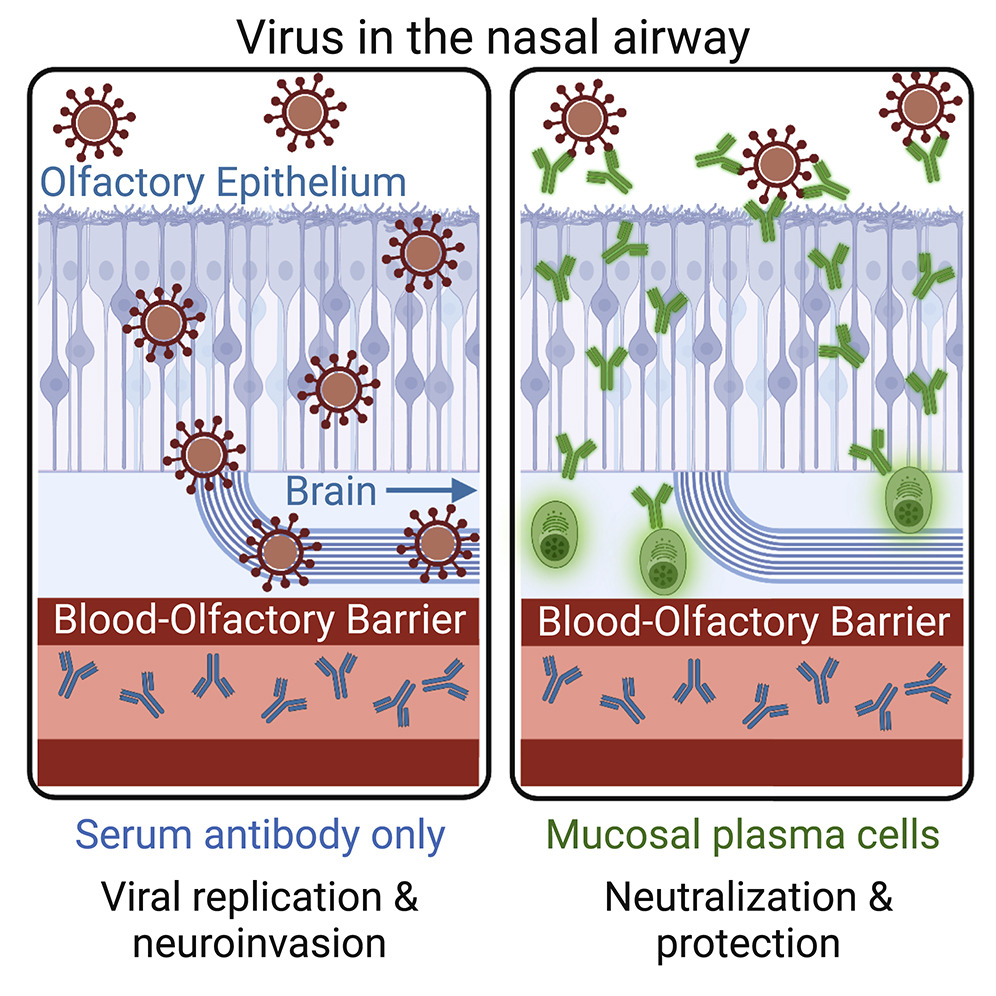
An aspect of the SARS-CoV-2 virus that is becoming ever more pertinent is the collection of chronic conditions referred to as ‘Long COVID’, which includes blood clots (Knight et al., 2022) and negative neurologic outcomes (Xu et al., 2022). Notable with such Long COVID cases is that it was not necessary for the patient to exhibit severe COVID-19 symptoms, nor to have been hospitalized.
The reason for this is likely that although the IM vaccines induce an immune response in the vascular system which often efficiently protects the body’s organs, this does not seem to provide protection for the olfactory epithelium, nor the brain, both of which can be infected directly from the mucosal tissues of the nasal passages (Wellford et al., 2022).
Although an infection with SARS-CoV-2 provides convalescent immunity (i.e. from fighting off an infection) within the mucosal tissues, this immunity fades over time, much like the immunity provided by SARS-CoV-2 vaccination. Since each infection comes with the risk of permanent damage (and death), the ideal way forward would seem to be to have an IN booster twice a year (matching the ~6 month fall-off in efficacy), that may provide sterilizing immunity.
Essentially this is why IN vaccines are increasingly being looked at as a possible way to effectively deal with such respiratory viruses, as they should provide much better protection for the individual, while also limiting community spread.
Making IN Vaccines Work
Despite what one may think with already three IN vaccines in use with (emergency) authorization, IN vaccines are not very common. Perhaps the most well-known attempt dates from before the SARS-CoV-2 pandemic, in the form of the FluMist vaccine (LAIV) which to this date is the only FDA-approved IN vaccine. This flu vaccine is notable for using attenuated influenza virus, rather than the inactivated virus of IM flu vaccines, and provides efficacy comparable to IM flu vaccines. Its main attractiveness is that it avoids the use of needles, and does not require trained personnel to administer the vaccine.
What is challenging with testing IN vaccines is the lack of standardized tests for mucosal immunity. This is largely due to IN not having received much attention, which makes running large-scale trials of such vaccines and assessing their efficacy largely unexplored territory for many regulators. Even so, AstraZeneca and other pharmaceutical companies are currently running trials for IN SARS-CoV-2 vaccines.
Whether or not an IM vaccine can be adapted to work as an IN vaccine mostly depends on the type. The sub-unit type of vaccine (e.g. Razi Cov Pars) likely requires an adjuvant in order to create a strong enough response, while adenovirus-based IM vaccines can basically be used as-is, since as noted earlier, adenoviruses naturally infect mucosal tissue. For e.g. the AstraZeneca IN vaccine trials that are currently ongoing, the challenge would seem to be mostly in defining the efficacy, in the absence of clear protocols and techniques.
Another challenge with IN vaccines is that the nasal mucosal surface provides innate protection against infections by forming a sticky trap that captures potential pathogens (Chavda et al., 2021). This is also why mRNA-filled liquid nanoparticles as used in IM mRNA vaccines do not seem to be a good match for IN vaccines. As these rely on having the body’s cells produce the target antibody from the mRNA, the lack of an effective way to get the mRNA into cells is a major hurdle, something which viral vectors by their basic design do not have to deal with.
Wait And See
With potentially billions of people across the world now having access to IN SARS-CoV-2 vaccines, there is the hope that this may do for the SARS-CoV-2 pandemic what the OPV did for polio in the 1950s and 1960s. Depending on the efficacy of these authorized IN vaccines, some regions and perhaps even nations may find themselves able to declare an end to community spread within a few years, if not less.
Meanwhile, Western pharmacological companies are still running their own IN vaccine trials that may deliver positive results by next year. All of which means that in the absence of an OWS-like push, Iran, India and China may provide us with the first glimpses of what a future with IN vaccines against respiratory viruses could look like as early as next year.
With some luck it may not only offer that much sought after off-ramp for the SARS-CoV-2 pandemic, but also provide IN vaccines with a much needed R&D boost. Who after all wouldn’t want a twice-yearly nasal spray that protects against even the common cold, or a more effective IN influenza vaccine?
Headline image: Untitled by Lauren Bishop for the Centers for Disease Control and Prevention













Standard comment. How if at all does it work on the immunocompromised? We have little immune system and the vaccine certainly doesn’t do much for me. But we are always left out.
Having less community spread by others would also help out those with an impaired immune system, wouldn’t it? In that regard IN vaccines may be just what those people need.
If you have little/no immune system, then things that bolster the immune system won’t be much good for you. That’s where herd immunity comes in. If most of the people around you are immune, then the virus can’t spread very efficiently and your chance of exposure is greatly lowered. It helps also if infected people isolate until they’re no longer contagious and exposed people isolate until they confirm they’re not infected.
I’m sure people will suddenly start acting for the good of the community any day now…
>That’s where herd immunity comes in.
That’s what they said during spring 2020. Two years later we still get sick, we still can’t buy no chips and economy is stagnating just like it had during Jaruzelski’s reign. To be honest, with each passing week I’m more and more seriously considering suicide because I’m an embedded engineer and nobody is hiring anymore. Thanks to covid, lockdowns and broken economy there’s just no work for ARM C and assembly coders where I live.
I’m not sure if you’re kidding or serious, so I’ll assume serious.
Please don’t commit suicide. Your life is valuable regardless of your job prospects.
Please talk to someone like Samaritans.org
Don’t blame covid, just blame lockdowns, and note that they were what broke the economy. Perhaps find the “experts” in your country who thought that locking down was a good idea, and who vilified sensible people like Anders Tegnell and Scott Atlas, and write them a bill for the harms their actions have done to you. You may well be able to collect enough money from those “experts” for the damage done by their criminal stupidity so as to move to somewhere where your valuable skills are still in demand.
One would think embedded is the kind of work that could be done remotely.
Not if you are embedded in an organization. Not clear what the poster meant by embedded engineer. The term has different meanings depending on context and industry.
Indeed and with ARM and C most likely it’s the “on chip” type of embedded.
I am one, and working remotely (well 60/40 but remotely today).
We are hiring too, so dragonborne, drop me a line.
I assume you are being sarcastic. I’m an embedded software engineer and it has never been easier to find a job. There is a huge shortage. The lockdown induced supply problem only increase the demand for engineering. It has nothing to do with the covid flu. I’ve had it three times. The regular flu is worse.
I have had a very difficult time this last few years as well amigo, and it would be a lie to say I haven’t had similar considerations. I won’t tell you what to do, but skipping steps never seems to help when I’m working on something, and I suspect that is true of debugging my being too lol. Good luck.
I don’t follow “I’m sure people will suddenly start acting for the good of the community any day now…” How does the good of the few equate with the good of the community? Seems like you are making an argument for the good of the individual, and not the good of the community. A “devil’s advocate” could argue that the few place an inordinate burden on the community and the community would be better off deploying the resources elsewhere.
I solved that problem by giving you are “wearable” secondary immune system, cover your mucosa with a modified probiotic (which is normally there in the natural form) that uses a receptor lure to trap and destroy viral particles. The Australian government, and others have known about it since April 2020. And I “open sourced” the entire thing, so don’t expect big pharma to get behind it.
There are other IN treatments that work even for them. Israel has approved what is essentially antiseptic for the nose that kills covid for 12 hours with one spray.
Herd immunity is all about providing protection for those without robust immune systems. However, IN vaccines using attenuated (not dead) virus like the IN flu vaccine can be dangerous for those with compromised immune systems, as exposure to these recently vaccinated individuals (and their nasal secretions) can be enough to cause disease in the immuno compromised individual. So, e.g., keep away from that person on chemo for a little while after getting your IN flu vaccine. Still a net positive if it reduces disease spread at a greater rate than IM vaccines.
How? Eight percent of our DNA consists of remnants of ancient viruses, and another 40 percent is made up of repetitive strings of genetic letters that is also thought to have a viral origin. It may be that we evolved to what we are by assimilating viral genetic code. One could argue that viral resistance reduces opportunities for further evolution.
To this I wish those biologists who hope to find dinosaur DNA and reintroduce dinosaurs 🦕; “Good Luck!”
Those hatchlings will not last a day before getting infected by a dozen ancient diseases of which they have no immunity.
I feel like this will eventually lead to a replacement of IM vaccine by IN.
I would rather have both. And anything else you can give me that might help me against any disease, thanks!
Never seen the Borg get sick.
Capt. Janeway destroyed the Borg with an infection.
Hugh and 7 of 9 both had health issues, Picard “Locutius” suffered from old age, headaches, etc.
Ha I’ve been re-watching Voyager and just saw that episode.
Yeah—the reason you don’t see sick borgs in the collective is that they consider it more efficient to simply salvage their cybernetic parts and recycle the biomatter instead of trying to heal them. You can just assimilate more eh
Excellent innovation! They are advancing from gaslighting to just gassing the public.
Nasal vaccines are a great medical innovation definitely, but we already have an off-ramp for covid and other coronaviruses, it is best described as “tolerating their inevitable spread”. Perhaps better to market this as a way to reduce the severity of flu seasons, rather than target it to a virus for which everyone has now seen the sense of the focused protection (Swedish) approach and simply learned to accept.
Because every virus humans have ever been exposed to has just mutated into non-dangerous, yearly events that we tolerate. It isn’t like norovirus, whooping cough, rabies, or polio still kill half a million a year.
Not every virus, but every respiratory virus. Respiratory viruses have evolutionary pressures which push for mild-symptoms-and-ultra-transmissible, unfortunately diseases which are waterborne (Cholera for example) or use other methods (Rabies in saliva, Norovirus via surface deposits and diarrhoea) are under no such pressures. But yes, as a general principle, tolerating the spread does work for respiratory viruses, it is atleast less damaging than trying to break the economy to stop them. Although, ofcourse, a vaccine which can make symptoms milder is always welcome.
Wait, is it safe to say the obvious out loud again? When did that happen?
Pfizer has paid the largest fraud settlement in history (in 2009, not long ago at all) and fakes their drug trials. FDA is complicit and is a captured regulator
The incredibly shady and exploitative oral polio experiment caused more cases than it prevented. The polio cases in NYC recently are descended from stock used in the oral polio vaccine.
With that kind of logic you should avoid cars, airplanes, furniture, food, clothing, fresh water, etc. All of these things have been made by shady people and all of them have killed people. Furniture kills more people than polio does.
You are onto something here. We should spend more resources making furniture safe and worry less about polio.
>fresh water
prevents polio better than ANYTHING
Have you seen an iron lung recently? No? Then it was worth it.
Respirators have replaced Iron Lungs and Oxygen Tents.
>> Nobody knew what myocarditis was two years ago.
I’ve known what myocarditis is for decades, and I’m not a medical professional. Many things can cause myocarditis, including numerous viral infections – 3 per 1,000 for individuals hospitalized with COVID-19, including both vaccinated and unvaccinated individuals, will develop it. The vaccines may increase the risk of myocarditis among a segment of the population, but the corollary is that reducing your chances of being infected with COVID also reduces the risk of myocarditis.
Data please? Seems counterintuitive vs. “Many things can cause myocarditis, including numerous viral infections” and “3 per 1,000 for individuals hospitalized with COVID-19, including both vaccinated and unvaccinated individuals, will develop it.”
Myocarditis, pericarditis, and blood clots resulting from vaccinations might be prevented by correct injection technique. Aspirating the syringe – pulling back before injecting – indicates whether or not the needle is in a blood vessel. If blood is drawn, that dose is discarded and a new injection site is chosen.
There is experimental proof in mice that injecting Covid vaccines into blood vessels reliably causes myo- and pericarditis and clots. This is pretty strong evidence that doing the same in humans is at least partly to blame for the devastating effects some people experience after being vaccinated.
Sadly, medical modernists have decided that aspiration is unnecessary, thereby discarding many decades of sound medical experience and possibly dooming people to needless suffering. I’ve spoken to a few older / retired nurses, one low-side-of-middle-age doctor, and my pharmacist about injection technique. They all agree that aspiration is necessary – yet the practice is disappearing. In my mind, this is inexcusable.
Despite the very low incidence of serious adverse vaccine reactions, I’m holding off on my fourth shot in hopes of finding someone who will aspirate. My age and pre-existing conditions mean that I’m likely to either not survive, or not want to survive, an adverse reaction. For me a viable IN vaccine can’t be available too soon.
Actually was the opposite of “safe, highly effective and stopped transmission” here and their lies cost was a family member and our psychical health.
I notice an absence of any information as to WHY these type of medication are as good as never approved. And I’m sure there is a damn good reason.
But perhaps we aren’t even allowed to mention such things anymore?
I noticed the same on wikipedia on a few subjects, with suggestions that some thing is ‘perfect’ and yet in decades was never approved in ANY country. And they almost never delve into why not. And people don’t even put 1 and 1 together when that happens but happily crow all over the internet (and TV) that something is so ‘perfect’.
Do you have any particular examples? When a drug is submitted for approval, all test data must be disclosed, both good and bad.
There can be any number of reasons why companies don’t disclose data. Do you publish every line of code as you write it? No, you throw some of them out and nobody sees them. Companies do the same with their failed experiments.
Do you really think that the average person believes it when it’s said thay something is “perfect”? “People say…” is a very poor way to argue.
You are suggesting that they were submitted for approval, but maybe the results were so bad that the submissions never came.
I used to think that the average person was really smart, then I heard people that seemed to be much smarter than average say dumb things. Now I think that even smart people are at least sometimes dumb. I’ll leave it to you to deduce the average level of intelligence.
well its not ‘never approved’. These IN vaccines for covid have been approved in china and india that I know of, could be others as well. Why they aren’t approved here often comes down to money and time needed to go through the testing and approval proces. Most FDA approvals take 5+ years, yet we’ve only been in the covid-19 pandemic for 2.5 years. Many processes had to be specially handlheld and run in parallel, risking a lot of capital in order to get the vaccines we do have approved in time to us good. They didn’t just change all approval processes to do the same, and covid research just isn’t reciving that evel of emergency priority now.
It’s called “follow the money”
You’re onto something here.
You must remember, often media greatly exaggerates the potential of a new medical advance – the vast majority of potential drugs don’t make it through the process. I don’t think any credible source describes any medication or medical intervention as “perfect” or “miracle” – those words are usually from media with an agenda (I mean just look at how silly the whole Hydroxychloroquine/Ivermectin debacle was). The only people who “crow” over some new magic drug/supplement/treatment are those who are either trying to make money from it, or using it to promote their own questionable ideas of diet/lifestyle/religion
Where’s the hack? Well there’s plenty of hacks in the drug trials if that counts
I think the ship has sailed on widespread adoption of new covid vaccines. The governments have told too many lies for too long, making claims that don’t align with their own scientific literature. I’m sure my wife and I aren’t the only people that went into the pandemic generally pro-vaccine and who came out vaccine skeptics.
No medical treatment is perfectly safe (especially a very new one), and if the government won’t admit that, what else won’t they tell us? Also not being able to discuss something openly without being censored is the red flag of all red flags.
They are obviously being controlled by the lizard people of Mars, but you never hear about talk about that without being shouted down – coincidence, I think not!
Stop spreading conspiracy theories without proof. Governments are known to be systematically incompetent, kowtowing, simply corrupt or exploitative, etc.
Kind of making my point for me…
Spoken like a true lizard-person, I’m not afraid of your moon-gulag!
The first part was a joke. The second part is a fact.
I’d agree. And then you get some joker who uses fallacies/’jokes’ to misinterpret your valid points. Wether he is conscious of it or not is sadly beside the issue. Your valid points and his fallacies are tossed into the ‘looney’ basket as a whole.
Seems like politics has innoculated itself against critism.
As long as proper free choice is given so that informed consent is possible then risks are ok. the trouble is throughout this pandemic coercion has been used instead. If we’d stuck to respecting informed consent then there’d be a lot less problems nowadays than there are.
Stop making the problem (in a govt funded lab) and you wont have to come up with fixes
I assume you are being sarcastic. I’m an embedded software engineer and it has never been easier to find a job. There is a huge shortage. The lockdown induced supply problem only increase the demand for engineering. It has nothing to do with the covid flu. I’ve had it three times. The regular flu is worse.