
As areas of uncontrolled cell growth, cancerous growth form a major problem for a multi-celled organism like us humans. Thus before they can begin to affect our long-term prospects of a continued existence, eradicating these cells-gone-wrong is essential. Unfortunately, doing so without affecting healthy cells significantly is tough. Treatments such as chemotherapy are correspondingly rough on the body, while radiation therapy is a lot more directed. Perhaps one of the more fascinating treatments involves ultrasound, with the IEEE Spectrum magazine recently covering one company providing histotripsy equipment.
Ultrasound has found many applications in the medical field far beyond imaging, with therapeutic ultrasound by itself covering a variety of methods to perform actions within the body without breaking the skin. By using high-energy ultrasound, everything from kidney stones to fat cells and cancerous cells can be accurately targeted and destroyed. For liver tumors the application of so-called histotropsy has become quite common, allowing certain types of tumors to be ablated non-invasively after which the body can handle the clean-up.
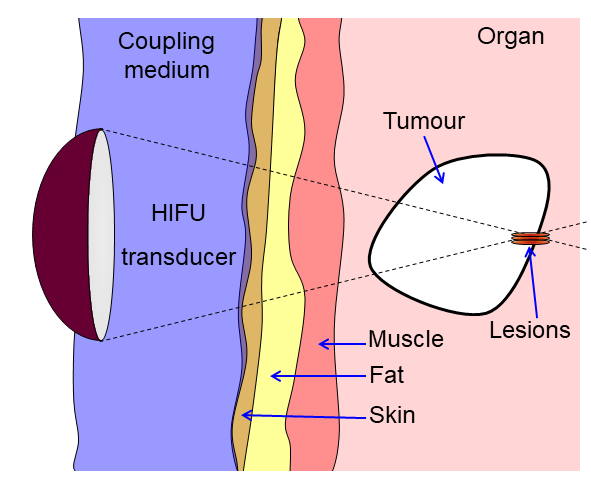
Histotropsy is a form of high-intensify focused ultrasound (HIFU) that uses either continuous or pulsed waves to achieve the desired effect, with the HIFU transducer equipped with an acoustic lens to establish a focal point. In the case of histotripsy cavitation is induced at this focal point that ends up destroying the local tissue. Beyond liver tumors the expectation is that other tumors will soon be treated in a similar manner, which could be good news for especially solid tumors.
Along with new approaches like CAR T cell immunotherapy, the prospects for cancer becoming a very treatable set of diseases would seem to be brighter than ever.












I am kinda interested in knowing who actually drives research in these medical tech that leads to the invention/creation of equipment that doctors use. I mean how were endoscopes, CAT scan, MRI etc first developed? Who wrote the “requirement” document?
I just find it kinda hard to believe that there are full time doctors who are also electronics hobbyists trying to solve problems in their fields? Because that’s the only way I can fathom the developments. I mean you DO have to experience these complex problems firsthand to be able to think of a way to solve them, right? Take the example of dentistry. You just know, the first dentists must have also been tinkerers who built their own tool like those weird metal pick things, same with orthopedicians of the old they likely knew basic metalworking to make braces for legs etc. Or at least they communicated this to a metalworker
Sorry if I’m too verbose. I just couldn’t think of another way to explain this.
Most of the time it’s trial and error, often done by poor inventors in places like India, Pakistan, Cambodia or Tajikistan. Nothing to do with being particularly smart or educated. For example first MRI machine was built in Udaipur by a man who used to run his chicken farming business and his father was persecuted by the British.
Nonsense, the principles of NMR were invented by an American physicist in 1930s, and the application for medical imaging was inverted by an American physician and inventor in the 1970s.
Explain to me how some chicken farmer without an education in physics could possibly theorize or build something as incredibly delicate as an MRI machine.
Those poor inventors can weld a rusty car back together with an improvised transformer, and sometimes somebody dies. That’s impressive given their situation, but don’t pretend they invent groundbreaking things every day.
Can you provide any support for this claim about the MRI? The usual names listed are Raymond Damadian, Paul Lauterbur, and Peter Mansfield. The first two are Americans, Manfield is British. All were academic researchers. Lauterbur and Mansfield were awarded the Nobel Prize for the development of MRI, which led to controversy over the exclusion of Damadian.
History of science and especially of medicine has become an increasingly popular field of research since the 1980s, and it does cover the modern era (XVIth century and beyond) where instrumental techniques, medicine and other fields of scientific research started to match and intertwine. You should find a lot of free papers online to start answering your questions, and some very good books aswell.
I was working for an ultrasound company that was doing stuff related to this. They were just doing imaging and then one of the developers read a journal article about ablation and they started building higher power units and trying to see if they could do ablation with them as well because they thought there might be a market for it.
But most current research is done through universities because most commercial firms won’t spend the time and money on something unless it has a quick, definite path to profitability. Much of the time, small university-created startups will take university research and try to develop it and then get purchased by a big company once it looks promising.
A great read on the development of MRI is “A Machine Called Indomitable” by Sonny Kleinfield. Most of these transitions are….. hey, that looks cool. I wonder if I can do this with it?
Usually not planned, just piddling about. When we piddle though, the IRB keeps close watch to make sure the risks are adequately addressed.
Big pharma/big pharam tech. 🤷♂️
Big scientific project often offshoot such techology… take a look at CERN discovered tech used everyday now, in medicine and elsewhere… these laboratories are not usless research about raw physics…
My dad (physics prof demoted to chemist when he crossed pond) did some basic research with using NMR to detect decomp products in teeth in the ’60-’70s.
Before he died, he met some people who had built tiny NMR devices at an ACS meeting, but didn’t have an application.
He pointed them to the old research on screening for tooth decay.
No more routine dental x-rays, perhaps.
Well.
I’m an MD/PhD physician-scientist. I’m a full time clinician (70+hrs a week usually!) which doesn’t leave a lot of time at the bench. I can tell you that about 50% of us get the degrees then don’t do proper bench research (mine was biochem/mol bio focusing on virology and antiviral development) ever again, but most of us at least end up in academia and have official or unofficial research requirements for promotion. Plus we like it anyway. Usually clinical research rather than basic science though (like me, now). In some specialities like radiation oncology, the majority of them are MD/PhDs and in any case, there is still a huge number of us going at it in many different specialities- yes as EEs, biochemists, etc. Now I could talk forever on the subject, but the degree to which your institution supports this varies widely. During training a lot of of program have semi-extended residencies or some have a built in research year anyway. At one of my institutions the surgeons all worked in a fetal sheep lab doing … something… for their research year.
.
Some departments/institutions are very pro-development (of devices, drugs, etc) and by that I mean “still pays you when you work in the lab” and that is negotiated. Usually the agreement is similar to “regular” PhDs in that you have a time period in which you get paid by the department but then are expected to secure grant funding. Some HUGE clinical departments (surgery, etc) have a small group of PhDs within the department with no clinical obligations that work strictly on basic science, or MD/PhDs (or less frequently MDs without formal PhD but still crackerjack basic scientists… you don’t need a degree to be a good scientist!) that are paid from the department without grant funding requirements. Those gigs are more rare, for obvious reasons.
.
hope that helps a little.
I think in many cases it isn’t driven by a need from the medical field, but someone working on some kind of technology thinking “maybe this could be useful for doctors”.
Sometimes, a solution in search of a problem isn’t a bad thing.
CAT scans had several critical bits of development. Austrian mathematician Johann Radon developed the transforms underlying the “computed” aspect of CAT in 1917. Tetelbaum and Korenblum in Russia (1957) made important contributions, as did Allan Cormack in South Africa (1963-1972). Godfrey Hounsfield at EMI in Great Britain was instrumental in the creation of the first CAT scanner (1971-1972). The EMI development was funded by EMI’s profits on the Beatles and then UK government contributions. The EMI machine was a head scanner; the first full-body scanner was developed by Robert Ledley in the U.S.A. (1974). — from wikipedia.
Im no doctor. Im certainly not qualified to evaluate nor criticize this science. BUT Id be terribly concerned if my doctor proposed blasting a tumor with ultrasound. It really seems like a great way to turn one localized tumor into a traveling circus of cancerous cells spreading across my systems.
Hopefully some of these mRNA immunotherapy pathways are solid and robustly proven before some doctor starts spitting the C word my way. Im way more comfortable with that idea than BLAST the cancer away.
Are you, like, stupid? I mean really, this is proven medical technology, effective, save, but just because you, a random tech-site visitor are “concerned” for no reason other than your imagination, you feel the need to type some incredibly daft nonsense?? This isn’t X my man.
True of most cancer surgery.
Cutting it, makes it spread.
They generally start with chemo, to weaken the cancer cells, then cut.
Each cancer is it’s own thing though, why they make the big bucks.
I’d assume something similar with this.
I feel obligated to comment and disclosure- I’m not an oncologist, but am a real life different kind of doctor and deal with onc alllll the time.
1- Ablation of tumor though non-surgical means is very common a number of ways. Chemotherapy (systemic obv) but also localized (such as injecting into cerebrospinal fluid) or the peritoneal space exists too as “common” modalities.
2- Things like radiation therapy (directed such as Gamma Knife, whole body to kill bone marrow, everything in between) similarly exists. Usually (and again I’m a little out of my depth on the specifics) the goal is to “shrink” the tumor if it is a solid tumor but I believe the mechanism isn’t so much kill the tumor as kill the blood supply feeding the tumor, then the tumor necroses. Viola- shrinkage.
3- certain cancers have a propensity to either stay put or some metastasize widely. Some “benign” stuff also spreads so even for me it gets confusing fast.
4- tumors as most people think of them are rarely an isolated, well differentiated mass, ball, wad of tissue, whathaveyou. Those that are are very easily and definitively(cured) treated surgically. THe rest of it … it isn’t a solid tumor like you think with distinct margins. The cells sort of spread out in a histogram distribution (glioblastoma, for example) so you can’t really remove it surgically because there isn’t an edge really …
5- thus chemotherapy etc.
But if you’re doing this on a cell by cell basis (the agitation of the cell wall causing destruction of the cancer cell itself), the cells that can spread and cause tumors in other locations can’t spread. Or less of them would. I would expect they would use this type of treatment on tumors that tend to be stationary and not subject to moving to other areas through the pathways of the body.
And if you start at the center of the tumor and work your way out, destroying cells the entire time the number of cells you’d miss would be smaller.
They’re getting pretty good with these therapies (gamma knife being an example), so I have confidence this is yet another tool in the arsenal to defeat cancer. Having lost too many people to cancer, I’ll take whatever they can do to prevent losing another person.
I’ve done the software for a couple of medical devices (and some aircraft devices).
Typically it’s a small company started by a doctor (or a small group) who’s technically literate but doesn’t know the details of electronics or software. Or casing. Or ergonomics. He knows what’s possible, but doesn’t have the expertise to make it.
Also typically it’s someone who did graduate research in medicine, got a “proof of concept” working in the lab, then left to start his own business making the product. He gets some seed money, sets up a small lab/production area, develops a product, then goes for FDA approval.
(Also typically, angel investors give seed money in return for stock, if the product is successful they take over the company and boot the founder, then install their own managers. The founder (also with lots of stock) is rich, but no longer has his company. Lots of doctors are running their second company using personal funds, having lost their first. But I digress…)
For aircraft, the FAA has something called a “DER” (Designated Engineer Responsible), who is someone in the field that knows aircraft and whichever technology, they are hired to oversee the technical details of the development while the FAA people worry about the bureaucracy. Also, sometimes pilots come in and make suggestions during the development process.
So for a small medical company there are doctors who know everything there is to know about blood, know how this new blood sensor they’ve developed works, and hire engineers who know about safety certification (software, hardware, mechanical) to make it into a product that detects how close a bag of blood is to going bad.
^this
This wikipedia article discusses the key players in MRI development, but it also shines a light on OP’s question: https://en.wikipedia.org/wiki/History_of_magnetic_resonance_imaging
As a side not, ultrasound services are mostly hated by the US healthcare insurers. Some are not, but the ones I’ve run across were (prenatal ultrasound – 100% refused coverage no matter who you ask or why).
Is there perhaps a deeper unknown story we should be aware of? (us, who paid for the said services with our cash).
On the topic of research … same … if there are grant moneys, there is research, no moneys, no research, only unofficial volunteers (and all kinds of magic crystals’ healers, or pebble placers, you name it).
I am pretty sure in some particular cases and in some very specific occasions ultrasound can do stuffs that the other therapies won’t. I am also pretty sure ultrasound treatment can complement other therapies or vice versa. I am just not sure it won’t be suddenly and irreversibly banned in the US for no apparent/good reason.
As a self-appointed delegate for the profession (caveats blah blah of course I’m biased, The Man, I inject microchips in fetuses, whatever gimme a break here public..)
Can I ask- what do you mean by prenatal ultrasound? I don’t mean to pry but … do you mean before pregnancy? Or of an existing pregnancy? The distinction matters a lot. I am certain fetal ultrasound is standard of care to assess many things like head circumference, nuchal thickness (a trisomy indication), fetal heart anatomy and a bunch of things. If that was denied… that is a big deal. But if it is before pregnancy, I’m less informed but that isn’t really standard of care in the US, where the entire assisted fertilization thing is really hit and miss. And highly suspected diagnosis dependent. Some of it is covered, some not and highly subject to local practice standards and even individual physician standards and practices. As you seem to be painfully aware.
.
There is no deeper unknown story. But again, I’m The Man, Of Course That’s What I’d say, I’m a shill for Big Pharma… take your pick. Research is expensive, grants fund most of it, others of us do it free because it’s interesting to us, clinical practice is boring and redundant, and yeah there are tons of snake oil salesmen but most “real” research (it is not hard to distinguish) is imperfect but still quite good. Facebook and insta are not vectors for science.
.
Finally. Ultrasound is, at this point, purely 1) diagnostic 2) non-ionizing radiation and as close to zero risk as anything we have 3) definitely is the imaging of choice for a number of suspected pathologies due to #2, and can 4) absolutely do things xrays, MRI etc cannot do. Often and way better. All the time. Daily for me personally. Specifically, dynamic, live, 3-d imaging such as heart valves for patients undergoing heart surgery.
.
There is no big conspiracy I’m sad to say (see my excuses above). There are no ultrasound therapies that I’m aware of in standard use that are efficacious. Only diagnostic imaging.
best
NO apologies needed, if I am wrong I am wrong and I am not a doctor (though, have a relative who majored in both gynecology and pediatrics, teaching professor, author of textbooks, etc etc – so a backdoor to a real knowledge).
Pregnancy ultrasound, of course, not before, which about shows my arrogance, and, to tell the truth, remembering all the proper lingo was never my strongest skill (database-ing and programmi-ring are, hwoever spelking dast eez).
I second your opinions in the third paragraph, which was backed my many doctors that I’ve personally asked. Any non-ionizing radiation is harmless, but I live in the state of Delaware that protects Big Profits first, Big Corporations second, and average Sam needs – usually not at all. Here’s where my speculation goes – it looks like someone somewhere might have sued for what was mistakenly attributed to ultrasound, so now it is no longer covered in Delaware. I also think that this could be inline of the still ongoing (and rather unfortunate for the rest of us) scare that certain vaccines cause autism, hence, some parents opt for no vaccination for their kids (thus, making sure eradicated diseases indirectly restart anew).
Man! That is insane. Even ACOG (am col of Gyn) recommends 1 standard ultrasound exam. That super sucks. My interactions with the US health care system from the patient side have been unencouraging. And lead to self-loathing for being part of the problem.
I’ll have to point out another tidbit.
I was born and grew up in rather rural place where doctors and nurses were half-trusted for the simple reason that some of them went into the profession for quick buck, but that wasn’t the only reason – some bribed/bought their way through college/university, so, obviously, they were the wrong people in the wrong place, and since this was USSR with its “planned economy” where grads were “appointed” to far away places (sometimes against their will) they were literally stuck, they hated their jobs, and they hated their patients. (as a side note, changing careers was not that easy – there was a law punishing for being unemployed – wonders of planned/forced socialism economy – so one couldn’t just pick up and quit his/her job – he/she had to jump through legal hoops, and, obviously, with bribes it was easier).
I am explaining this, because this is important – people who lived in such places tend to distrust doctors, and they would be the ones avoiding needed exams and procedures, and turning to friendly quacks, shamans (btw, don’t I have a true story from the relative I’ve mentioned in the first paragraph – she taught in India, and had witnessed their “prenatal care” system for the poor, but I digress). What happens next is even worse – these people tell their kids “doctors are in the profession just for the big/quick buck, and some, if not most, destroy your health deliberately, so that they’ll have a job.” I am not making this up : – [
We have a large patient population matching your description above and let me tell you, as a human, it is pretty hard to master your emotions when you are taking care of someone’s kid, family, whatever and you get distrust at best (are you even a doctor?) and outright hostility more often (you aren’t touching them, I’m coming back into the OR with all of you to make sure you’re doing your job…. Ummm, no). I’m a man, too, (nominally hahah) and don’t even have to put up with the overt sexism and racism I’ve seen first hand. I’ve heard your story a bunch ( we also have nurses, etc from the same background and they have been amazing at informing me and helping me understand this) so I like to think I have empathy and respond kindly and with understanding but… boy. It can be hard.
As another side note, observing the ultrasound machines (that I’ve personally seen) in action, I was always wondered just why are they not built like MRIs, ie, entire 360 degree view, and why are they seem to be rather simple continuous radar ping type. While it may be good enough for a professional with decades of experience, I would honestly speculate that layer-by-layer 360 degree would make a true 3D representation, and thus be infinitely more useful.
Diagnostic imaging, yes, but things are now in the 21st century, and there are amazing 3D reconstructions that can cross-match things quite well. For example, I always wanted to know just how the Krebs Cycle works in my body (not in a textbook example), from which organ to which organ this and that, etc. I am sure it is way too advanced of a topic to just put in a Power Point (no, I never use it it home, btw, but at my work I am regularly required to pre-chew and pre-digest complex/sophisticated things in the Power Pont naive/manager level), but I am always eager to know.
Few more things.
There absolutely exists 3d Ultrasound. We use it for heart valves, fetal ultrasound, all kinds of stuff.
But think about it. We also have regular old 2d xrays that we use allllll the time despite the fact we also have amazing 3d reconstruction CT scanners, MRIs, and so on.
So your base assumptions are… off base a little. We have them, but for a lot of things the boring old 2d is not just adequate but better, as well as cheaper and easier. Triple win!
If you are thinking about imaging for krebs cycle etc, consider the wavelengths of sound (big), light (variable) xrays (smaller) etc and that the only way we have to image small things is when the imaging medium is… smaller. So like you need an electron microscope (also definitely a thing).
If i’m not totally misreading your comment, I would suggest if you are truly interested you can go to a junior college and for like $40 (maybe a bit more… I was at JC 30 years ago almost) you can take an intro bio course. I’ve done adult education it is amazing.
Roger that, and I thank you for taking time explaining things at the curios amateur level.
I am always eager to learn anything and I sure need proper homework done (intro) before embarking into advanced stuffs.
One particular (midly related) talk that piqued my attention was “An Introduction to Quantum Biology – with Philip Ball” – but that wasn’t the rabbit hole that swerved me in, the rabbit hole was one very interesting observation (not mine, sadly) that cancer growth in humans seem to be reverse Krebs cycle, and in itself there is nothing wrong with that, since it is how plant’s biology works, reverse Krebs cycle (my oversimplification). It also goes deeper than that, since neither one (forward or reverse) Krebs cycle doesn’t seem to be “programmed” in any genes per se (again, my oversimplification), however, reverse Krebs cycle is present everywhere, viruses, plants. The speculation goes like this, since the reverse path is actually kind of sort primordial way of metabolism, in some way cancer cells simply restart their ancient cycle anew.
I think this about explains the depth of the rabbit hole I ended up in. I’ve run all this by my relative and her reply was “sure, but just WHY you want to know these things? You won’t be able to solve the cancer riddle, and in the end would end up more confused than self-educated, but feel free to prove me wrong.” : – ] We are on good terms, so this was gentle humor – I regularly make fun on her, too, especially when/if she talks about AI and computers general.