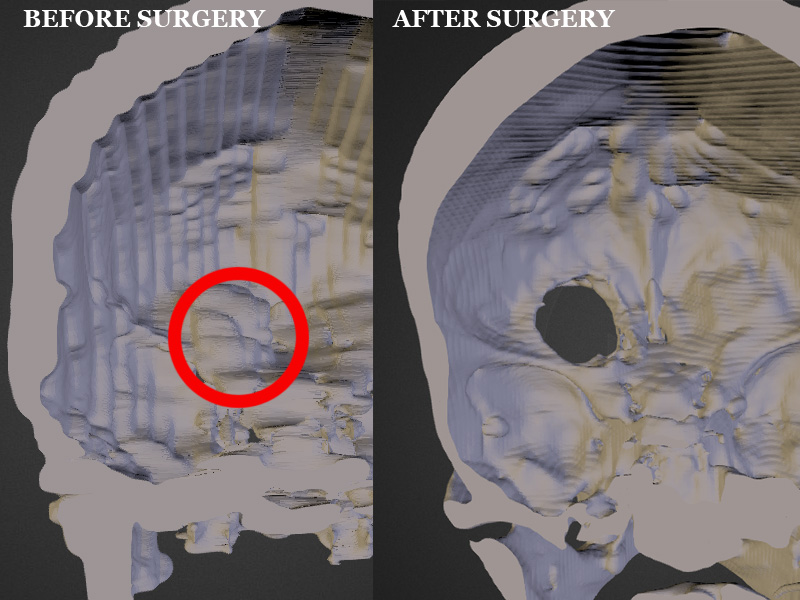
[Michael Balzer] shows us that you are your own best advocate when it comes to medical care – having the ability to print models of your own tumors is a bonus. [Michael’s] wife, Pamela, had been recovering from a thyroidectomy when she started getting headaches. She sought a second opinion after the first radiologist dismissed the MRI scans of her head – and learned she had a 3 cm tumor, a meningioma, behind her left eye. [Michael], host of All Things 3D, asked for the DICOM files (standard medical image format) from her MRI. When Pamela went for a follow-up, it looked like the tumor had grown aggressively; this was a false alarm. When [Michael] compared the two sets of DICOM images in Photoshop, the second MRI did not truly show the tumor had grown. It had only looked that way because the radiologist had taken the scan at a different angle! Needless to say, the couple was not pleased with this misdiagnosis.
However, the meningioma was still causing serious problems for Pamela. She was at risk of losing her sight, so she started researching the surgery required to remove the tumor. The most common surgery is a craniotomy: the skull is sawed open and the brain physically lifted in order to access the tumor below it. Not surprisingly, this carries a high risk of permanent damage to any nerves leading to loss of smell, taste, or sight if the brain is moved the wrong way. Pamela decided to look for an alternative surgery that was less invasive. [Michael] created a 3D print of her skull and meningioma from her MRIs. He used InVesalius, free software designed to convert the 2D DICOM files into 3D images. He then uploaded the 3D rendered skull to Sketchfab, sharing it with potential neurologists. Once a neurologist was found that was willing to consider an alternative surgery, [Michael] printed the skull and sent it to the doctor. The print was integral in planning out the novel procedure, in which a micro drill was inserted through the left eyelid to access the tumor. In the end, 95% of the tumor was removed with minimal scarring, and her eyesight was spared.
If you want to print your own MRI or CT scans, whether for medical use or to make a cool mug with your own mug, there are quite a few programs out there that can help. Besides the aforementioned InVesalius, there is DeVIDE, Seg3D, ImageVis3D, and MeshLab or MeshMixer.












You may also want to check out 3D slicer at http://slicer.org/ . It can handle DICOM natively and will export to STL. The learning curve is a bit steep but there are many tutorials available.
Every time I used Slicer with my DICOM files it crashed. Would not recommend.
“Necessity is the mother of invention” as they say. Perhaps Med school should be revised to include a semester of hacking and computer science. I’m glad that this had a happy ending. I hope all goes well from now on for you guys.
That link to the 3D visualisation of her skull (https://sketchfab.com/models/2dab8ac4176f4710a7269d5226878c21) is really interesting.
Very cool story.
Believe it or not, a lot of doctors going through med school are often idiots technologically speaking. I previously worked for the IT department for a very reputable medical school and was baffled how many Fellows could barely use email.
In most parts of the world, “fellows” imply people who have accumulated a minimum of 5 years university and a further 6 years specialising in what they do. By the time they return to Med School to teach they will have spent 10-15 years at the cutting edge of their fields. To say they are idiots because they can’t use a system you set up and/or we’re responsible for, in a manner at all confusing to people who came out of high school with better grades, better social communication skills and probably better partners 30 years ago is insensitive.
I could easily say; “Believe it or not, most of the guys from IT at the hospitals I work with are idiots and won’t install the right software or let me hook into the database so I can pull the Dicom files directly into …”
Insensitive insults aside, there are reasons technology like this isn’t used as often as would seem are a mix of practical, ethical and professional.
The simplistic summary
– we know that the way we do it usually, usually works (and have done it enough times we know how often it doesn’t)
– trying new ways is often risky, we don’t know what those risks are, it’s unethical to try radically new things on people to try out, and if we do stuff up, armchair lawyers and doctors are so tightly latched to our backsides we’ll abandon ship at the vaguest hint of difficulty.
I believe that if you can’t understand the real world at the same time that you are pursuing one degree after another is an issue. Call it Asperger”s syndrome or something else. They need to be able to think outside the box. A Dr. the is technically rounded Vs. one that just has pursued multiple degrees will make a much better surgeon in the real world. Theory is one thing, action is another.
I was wondering how one would remove a 3cm tumor with a micro drill, but that link says 3.5mm
Cudos to [Michael Balzer] for being such an effective advocate for his wife’s care and treatment.
Medicine isn’t to the point it needs to be to provide the best treatment for every patient. The push and the need points to personalized medicine, but the insurance companies push for evidence based medicine. I personally don’t think evidence based medicine will ever get us where we need to be. If we applied the standards of evidenced based medicine to everything parachutes would not be allowed when jumping out of airplanes due to the lack of controlled studies.
As a result we all have to be our own advocate.
Great example of love and how to be an advocate.
Sorry but your comments are a bit uninformed.
Up until the 60s we pretty much did have direct to consumer medicine. Then Thalidamide. The modern equivalent it complimentary “medicine” where individualised care is given but there is doubt about its effectiveness.
Oh, and parachutes are evidence based. Evidence based does not mean phase I – phase II – phase III – phase IV – randomised control trials with meta-analysis and postmarket surveillance – although that is important.
Evidence based means taking a rigorous scientific and statistical approach that is evaluated by informed and independent observers then translated into health outcomes.
After all, we have been using parachutes successful in practice for nearly 230 years now. Nonetheless parachuting has a known failure rate, and some of these failures result in unassisted landings. Certainly Juliane Koepcke survived falling from an exploding jet plane over Peru with only her seat.
(Black humour alert)
In World War Two, a randomised control trial was performed, with some crew falling with parachute and some without (either through not being equipped or being unserviceable); although it is undoubtable that a small number survived falls of several thousand meters, a greater proportion of those who opened their parachute survived.
(Some May argue the intention bias posed by those who were equipped with parachutes but failed to deploy them)
But basically, if you think that evidence based medicine has much to do with big pharma or insurance companies I have two things to say;
1) try looking north. Or south. Or east, or west, and in particular all those nations where Nixon didn’t sell his poorer voters’ health out to dry.
2) I saw a kid urinate in a reservoir – quick, it’s now sufficiently dilute that we can sell it to people as “urine therapy”. Seriously, google it.
(/black humour)
The parachute argument is old (circa 2006), and mostly misunderstood by pundits.
Respectfully,
Evidence based medicine is the criteria insurance companies use to deny many previously paid procedures. My argument isn’t against evidence based medicine being a valid scientific method for evaluating treatment methodologies, but the way insurance companies use it to deny payment and thereby exclude treatments to those that have ailments without evidence based treatments proven through rigorous studies funded by the pharmaceutical industry.
Yes, Nixen sold us out to Humana many years ago, but we sell ourselves short by not being open to new ideas and not trying to be better at what we do.
There’s a reason that even in countries with 100% socialized health care, evidence based standardized procedures are the norm: it’s cost.
If you want a highly specialized, patient tailored treatment plan the doctors treating a patient are going to need a higher level of training. Medical training is expensive. You’re also going to need more doctors, as their increased workload means they can individually treat fewer patients. Now you need more (presumably higher paid for their higher skill level) doctors. You’re also going to need a means of acquiring patient specific equipment and drugs — the cost of which is inverse to the number of patients it can be used for. Because of the unknown factors in a previously untested (at least together) series of treatments, the patient is going to require more followups, testing, etc. So now you need larger facilities, more equipment, more trained and pay-rolled staff, and so on. The cost increases exponentially the more specialized you get.
The technology and understanding of the human body needed to make that affordable doesn’t exist yet. There is no way to cheaply diagnose and provide intimately specialized care to a large number of patients suffering from an equally large number of diseases. It’s all about what you’re willing to spend.
I like the arguments but loads of cost savings can be had by eliminating unnecessary tests and treatments. following a flow chart in one size fits all medicine can be very expensive as well – if the flow chart says mri, thent he patient gets mri whether it would be useful for them or not.
Also, and even more importantly, smart people can do a lot of the legwork themselves- they have the time and motivation since they only have one patient and they care more than anyone about the outcome. Yet if a smart person comes with evidence having done their homework, even if they request cheaper tests and treatments, it is met with incredible resistance. Every roadblock is in the way of an educated individual who fashiions their own individually tailored plan for themselves.
the average joe doc is out of date on state of the art medical research- that’s not a complain- how could they possibly keep up with all the amazing reserach that is being done in every country on every medical problem. they only see things at best 5 years down the line, and sometimes not for decades. So if you’re life is at stake, and you want the best, you have to rsearch it yourselves. Docs should smile when a patient does this and be glad for the collaboration- but many are not.
so yes, if you want a third person to do individualized care for every cold virus, w’ere too big a group and it can’t be done. but its completely finanically affordable if one does it for themselves. (and i think individualized care can be improved in many cases even if not all patients are scientists).
In reference to the parachute argument, please reference this article in the BJM:
BMJ 2003; 327 doi: http://dx.doi.org/10.1136/bmj.327.7429.1459 (Published 18 December 2003)
Cite this as: BMJ 2003;327:1459
No studies found sufficiently randomized.
Indeed. A spoof arficle, Published in the traditional joke slot for Christmas. Im sorry i got the date wrong and i’m glad you pointed out that the hilarity started three years earlier than I remembered.
No edit button, alas, to make the circa 2006 more exact
I wont bore you with a more thorough rebuttal thsn this:
EBM randomised control trial
Customised care good care
When customised care = experimental care and you aren’t capable of being adequately consented because of preconcieved ideas at odds with your normal values = tragedy
I obviously do not know what personal journey you have gone through with this. Every time a patient dies, is injured or is otherwise worse off it is natural to seek meaning or attribute blame. Unfortunately most patients are not maligned. They are just unlucky. Ebm exists to make sure that part of that luck is not based on which doctor you live near, which company employs them or which government is in power.
But you can do worse than be given the internationally agreed standard of care for the majority of common and uncommon diseases.
For those that would like a longer rebuttal to the parachute issue, I recommend the following :
Satire, not spoof. The difference is that satire has a basis in reality, pointing out life’s absurdity.
There were actually two articles on the subject.
1. Smith G,Pell JP. Parachute use to prevent death and major trauma
related to gravitational challenge: systematic review of randomised
controlled trials. BMJ 2003;327: 1459-61.
2. Potts M, Prata N, Walsh J and Grossman A. Parachute approach to
evidence based medicine. BMJ 2006; 333:701-703.
The second agrees with your stated date.
But the point of both is that the search for truth can’t rely on only one methodology and the design of the study is important.
For example, a parachute is of no use if the fall doesn’t give it time to open.
I’m sorry your further rebuttal was cut out of your reply.
Outstanding effort and best wishes for sustained results. The guts to take personal responsibility to the next level and the courage of the surgeon to work ouside the boundries of typical procedures is commendable. Will never again think of the phrase “It isn’t brain surgery” in the same light.
From what im seeing they just knocked a hole in her skull without replacing the lost structure?
That story was a rollercoaster ride from start to finish. Glad to hear about the happy ending!
I don’t quite understand this: “95% of her tumor was removed”
Don’t you have to remove the entire tumor to keep it from regrowing?
Perhaps it means that 95% was removed flawlessly and there was only scarring from removal of the final 5% (that’s the happy ending I’d like to imagine).
It seems like it was a meningioma. Most are benign. They recur, but as long as they aren’t around one of the nerves, the spinal cord or get big enough to cause pressure/compression it is rarely an issue.
1-2% of autopsies have a previously unrecognised meningioma
It depend on whether it is malignant or “benign” , fast or slow growing. In this case the problem was from a slow growing benign tumor that was putting pressure on an optic nerve that would eventually cause permanent blindness in one eye.
I think it is always a comfort to know your surgeon/doctor has a 3d print out of your head. It is definitely relatively non invasive and gives more detail than images or 3d rendering on a screen.
I wonder if the inevitable published paper will cite [Michael] as an author or a footnote. I’ll bet on the latter, although that is still better than just writing that “a 3D printed model was produced.”
And now that the operation is over and a success he can drink wine out of his wife’s “skull” without having to worry about being constantly hunted by the police.
This. Is. So. Cool.
And it’s absolutely disgusting how incompetent those medicals professionals are.
This is absolutely awesome. Way to go man, really cool. Way to take you wife’s life into your own hands, instead of relying on other people that probably don’t give a shit, and are too cocky to say how shitty they are. That’s the problem now days, everyone thinks doctors are all the same, same intelligence, same knowledge etc, which is such bullshit. Would you think you local physicist at the community college is the next Einstein? I sure hope not.. Then why make the same leap when it comes to the medical field? Your all a bunch of ignoramus if you ask me. No cares about you except those who have proven they do, and the best are the best, and the person that probably got the job because there is no else to fill it, just like every other job, like management at corporations, or minimum wage employees, these people are no different, just the schooling. What does all that mean, you could take the same schooling and be just as intelligent as they are in medical areas. So then do it! They don’t care about you or their job, or helping people, or innovation, just money and greed.
“[Michael Balzer] shows us that you are your own best advocate when it comes to medical care”
Yeah, especially if you have massive amounts of economic privilege and access to high-tech resources.
All you need is the internet and a hacker mentality.
Oh for sure man. None of the things described in the post require time, money, education, connections, access to robust healthcare, etc. /s
(you really ought to think harder before commenting)
I didn’t realise that you could build models from CT scans. I thought it was just MRI’s. Now I’m gonna have to run off and find my mum’s CD of her spine.
It depends on what you want to print.
MRI gives better soft tissue recognition and can encode more than (essentially) density.
CT is better for most bones and moving objects expecially with contrast
Well this is from a spinal fusion. She has two rods and six screws in her lumber region. The CT scans are really clear on the CD they provided. Her vertebra were smaller than expected so the screws were too long and came out the other side. The surgeon fixed it after the scans revealed what happened. Bad for mum but makes for some great pics.
As interesting as this article is, I’m not sure why the internet has exploded with it these last few days, as this article was first published back on the 25th of Oct 2014, http://3dprintingindustry.com/2014/10/25/3d-printing-helps-husband-seek-treatment-for-wifes-brain-tumor/ nearly 3 months ago (actually there was one on the 19th of Oct, with much less info).
I had an head CT scan done a few months ago, and they gave me a disc with the dicom data on it, it loaded great into 3dslicer, but doing anything with it required a fair amount of RAM, and some of the other programme I tried were even worse. Nonetheless I do have an .stl floating around of my skull ready to 3d print one day when I’m feeling bored ;)
http://3dprintingindustry.com/2014/10/25/3d-printing-helps-husband-seek-treatment-for-wifes-brain-tumor/ kinda jumping on the bandwagon late? This was written about 3 months ago, still pretty cool though.
I had a head CT scan done a few months ago and used these programs to check it out, I found that you need a lot of RAM to really do anything easily, as some of them are extremely memory intensive and will just crash out if you don’t have a good enough system.