[Gui Cavalcanti], whose name you might recognize from MegaBots, got on a call with a medical professional in San Francisco and talked about respirators. The question being, can we design and deploy an open source version in time to help people?
Unnerving reports from Italy show that when the virus hits the susceptible population groups the device that becomes the decider between life and death is a ventilator. Unfortunately they are in short supply.
The problem gets tricky when it comes to what kind of respirator is needed CPAP, BIPAP, or Hi-Flo oxygen NIV are all out. These systems aerosolize the virus making it almost guaranteed that anyone around them will get infected.
What we need is a Nasal cannula-based NIV. This system humidifies air, mixes it with oxygen and then pushes a constant stream of it into people’s lungs. If we can design a simple and working system we can give those plans to factories around the globe and get these things made. If the factories fail us, let’s also have a version people can make at home.
If you aren’t sure if a ventilator is something you can work on there are other problems. Can you make algorithms to determine if a person needs a ventilator. Can we recycle n95 masks? Can we make n95 masks at home? Workers also require a negative pressure tent for housing patients. This will be especially useful if we need to build treatment facilities in gyms or office spaces. Lastly if you’re a medical professional, can you train people how to help?
Let’s beat this thing. The ultimate medical hackathon begins.












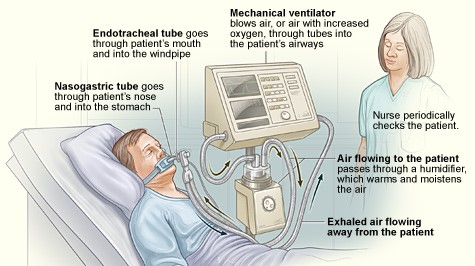
I’m an anesthesiologist/intensivt so I’m a specialist in mechanical ventilation. The device described in this post is not a ventilator but a high flow nasal cannula. The air is warmed and humidified to not dry out mucus membranes. Frequently sold under the brand name Optiflow and should be easy to construct, just bubble the gas through 37-40C water.
I was thinking just the same thing (Im only a biomed tech)
If I understand correctly, flow rates for the high flow nasal cannulae are quite high. The source of medical grade air or oxygen at these flow rates may perhaps be the biggest challenge.
Whats the difference between welding oxygen and medical grade oxygen? Does it really matter if the oxygen is not super pure?
Honestly, in case of emergency not really. They come from teh same process, and oxygen being so dangerous, must be filtered for anything that could spark and reaction.
Oxygen is NOT flammable if that’s what you’re implying.
I believe what he was implying is that welding oxygen HAS to be nearly as pure as medical one because otherwise it would be fire (explosion?) hazard due to contaminants inside pressure vessel.
Storm Raven: “technically” you are right but in actuality high concentrations of oxygen make otherwise minimally flammable things explosively flammable, and very dangerous. That’s why they have those warning signs everywhere it’s used.
Storm Raven: Below – is absolutely wrong. Oxygen is extremely flammable and is a bomb. Can explode just by friction. Needs understanding. Even at certain levels in a room may easily be ignited. Welders cannot touch fittings with dirty hands. Wrong gas mixtures are dangerous. With reasonable sense a respirator can be home made. Breathing Oxygen is safe. Special conditions apply for diving. Usually called Nitrox .eg. 32% or less Extremely poisonous below 30ft bar. and so on.
At Raul- Storm Raven is correct. Oxygen is not flammable. Oxygen is only a catalyst that without it you will not have a flame. Also, it does not make things more explosive. The explosively of the material depends on the chemistry of the material, and the mount available. Otherwise, every time someone lights a cigarette lighter, the whole atmosphere will catch on fire.
Zee and Storm Raven. A flame is caused by an exothermic chemical reaction between a hydrocarbon and an oxidizer. The O2 in this case is the oxidizer and therefore Oxygen is one of two reactants to be flammable. With your logic hydrocarbons are not flammable either in an atmosphere void of oxygen. Also, Zee, it is not a catalyst, as it is fully consumed in the reaction. Combustion requires only a hydrocarbon, oxygen and an ignition source. At the proper levels an explosion can be caused by static electricity.
I can’t speak for anyone else, but I for one would be perfectly happy to breathe welding O2 as long as it was passed through some kind of filter.
Another option for oxygen might be a device called a concentrator. They can be capable in real time of supplying more than 2 L/min of 95% O2 for as long as they have electricity to run off of (or more, I’m going by what my own unit can do), and they are fairly common devices on the market (even Amazon sells them, though I doubt those are medical grade ones).
I just said that an hour ago:
https://twitter.com/zoobab/status/1238109951027003392
“I remember @PHintjens in bed with a bottle of oxygen, as he had lungs cancer. Will go to Brico buy a welding torch with an Oxygen bottle, that can help #oxygen #breathing #MacGyver https://bricodepot.fr/catalogue/poste-a-souder-bi-gaz/prod13363/ ”
I am planning to weld my own steel bike frame with brazing (acetylene-oxygen). Gas can blow away the building though, you need to attach the bottles with chains. And there are local regulations about it as well.
Most of the modern mains powerd
Units will do 95% at 5lpm . The older units struggled at more than 3lpm
High flow oxygen therapy is in the order of 30-70lpm so unfortunately the concentrators dont cut the mustard
if i have options A. breathe welding o2 or B. dying by suffocating then pass me that bottle.
My understanding is that the oxygen used for medical purposes, and welding is not inherently different. There is a chain of custody for the containers designated for medical oxygen use that is not broken. They keep the tanks free of contamination. New tanks can be used, and then a new chain of custody is established and can be kept. My question is how much difficultywill be encountered in getting your tanks filled. This is all very interesting. Can an oxygen concentrator possible be incorporated in the design?
As a person with years of experience breathing welding supplies oxygen, I’ve never had any problems. Our fire department also filled all BA (Breathing Apparatus) at Airgas and such. No filter needed.
I am a Cryogenic Plant operator on a US Carrier. I produce liquid oxygen that is used for Aviators Breathing Oxygen (ABO) primarily. Secondary, the same liquid is also heated and converted to high pressure gaseous oxygen for medical use as well as welders. The oxygen is the same grade. Only difference is the system the high pressure cylinders are hooked up to for the ultimate use. Medical uses go to oil free and sterilized lines, where welders go to oil tolerant (not necessarily present) and likely dirty equipment.
Purity is rated at 94% or greater. Trace contaminants (Methane, Acetylene, Nitrous Oxides for example) are maintained below level that is suitable for use in ABO, and if contamination levels ever exceed, the liquid is dumped, tank is purged and refilled to yield a sat sample. I have never had a batch come back with levels that are unsafe in 10 years of operation in my plants.
Portable oxygen generators are there. why cant same be inbuilt into the ventilator to cut down the need of piped O2 and also the chance of explosion. The O2 gets made insitu and consumed then n there.
Oxygen DOES NOT explode. It supports combustion but by itself without a combustible fuel would only make the ignition source burn better and I suppose hotter.
As far as I know, the oxygen comes from 1 source and is all the same, the oxygen for breathing or diving requires the cylinders to be vacuumed cleaned before refill to guarantee certified purity, whereas industrial cylinders are just refilled as returned. Ive used industrial oxygen for years when scuba diving inc rebreather use for 5 years, with no ill effects, in cases of life or death I vouch use it
To avoid a fire, don’t use wax-based chapstick on the lips. The lips will dry out on exhalation. Was told by nurses in hospice to use KY jelly instead – a different application of its intended use.
Also, pure enough oxygen can cause the body to stop breathing. There must be at least a trace amount of CO2 in the bloodstream to trigger breathing. I am not in any medical profession.
I have gas welded since the ’60s, breath welding oxygen for headache. Not poisonous, it does not burn but burns other things. Problem with covid 19 is lungs get stiff, you need pressure difference to make breathing happen. If you don’t use oxygen, just air it may be enough? Need to find out. There are a few of us working on this already
There are different types of ventilators, from cpap to very complicated ones for intensive care. CPAPs simply provide slightly positive pressure to assist a patient who breathes autonomously and release professional respirators for more urgent cases. They are those used for night apneas. I designed and built one made from a plastic bottle, ultra-cheap and easy to make. Non-certifiable, to be used only in case of serious emergencies that justify the use of craft appliances and especially in poor countries could be useful. the problem is that I don’t know how to spread it. Can you help me?
This is quite amazing you’ve let a question oxygen Sidetrack and derail a whole conversation meant to help save humans all over the world, egos get over yourself move on to the problem thank you
MAX, I am trying to build a CPAP to combine with a full-face snorkel mask. Can you contact me with your method? I want it battery powered and portable. THANKS!
I’ve used welding oxygen when I needed it and was in the US and couldn’t afford medical oxygen.
I believe, that the Thrompe mechanism solves all the problems. Just need the water flow and you get pressurised air of great quality, no residues (oils) of pumps etc.
https://en.wikipedia.org/wiki/Trompe
Where I live it all comes from the same tank at the gas supplier’s. The difference is documentation and customer storage method. I’m happy to breathe out of my welding tank – just be sure it’s not acetylene :-)
Actually, acetylene was the very first gaseous pain relief. A whiff of the stinking stuff will make your head spin a bit, more is possible to cause death. Also wet sheets were spread over the op room table to the floor to control static ignition
Also, the three astronauts quickly killed in their lunar craft were doing 100% O2 (at 1/3 atmosphere pressure. Also, too much Oxygen is very toxic. Google before you leap!
There’s a difference that comes down to guaranteed purity. (I’m a biologist, I’ve bought different grades of oxygen.) But there are plenty of grades between welding and medical that are acceptable in a pinch.
There’s another factor, relatively minor but needs mention. Oils used for lubricating valves and such can be aspirated – I think it’s chemical pneumonitis? Lipoid pneumonia? I know of only one case, a scuba diver who had some oil inside the tank. An MD should know more.
Anyhow we could use industrial oxygen with a reasonably good pedigree – I have no doubt suppliers would gladly divert tanks for emergency use- and just be sure either to catch oil in baffles, or some other precautions.
I work in the industrial gas business and can tell you product is the same (liquid o2, almost each plant is medical certified) only the way they are filled into cylinders is different (different skids, more analysis)
This is my experience also (with high purity helium) .
If there is any standard lubricating oil in any part of the oxygen making process, you probably won’t be able to buy oxygen from that supplier as it’ll be a smoking hole. Silicone oil, maybe?
Attention, the equipment that handles oxygen at high pressure and extreme purity, must be free of oil or any other product that could catch fire. Raising the oxygen concentration and pressure can cause combustion at low temperatures even without spark.
i am a professional diver and dive medic technician. we are trained on treating patients in diving accidents in themixed gas saturation and air diving fields. there is no difference between breathing O2 and welding O2 gas the only difference is the bottle it comes in. medical bottles are coated so they dont rust and have to be checked regularly whilst welding bottles are not visually checked for rusting and particles to such a degree.
as for oil in the tank there is absolutely no oil at all in oxygen cylinders. the slightest amount of oil on any thread or valve would cause in instant explosion. all equipment that has to come in contact with high pressure oxygen must be free of oil or it will instantly combust. no exceptions. this is basic chemistry.
I confirm what Nathan sais; Welding bottles are only visual inspected; I also see that some say that high purity high pressure systems work without oil. That is not always true, there are many PTFE based oils which are tested and can operate at elevated pressure and temperatures (Fomblin, Kluberalfa, …) I believe they are also accepted in medical systems, again analysis will tell if the quality is sufficient.
“chemical pneumontis” may be evitable using sorbent tube filters. They will catch most VOCs from lubricants and aloow oxygen to pass properly. Finding an abundant supply of sorbent tubes may be a challenge. Another challenge is to determine the saturation of VOC in sorbent tubes before changing them, if used as filters. It could be estimated from sorbent tube manufacturer information and flowrates plus estimated contamination by lubricants (offgassing rates at temperature and pressures).
If you pass it through a bubbler there should be no issues with oils getting in the lung. Maybe 2 for redundancy.
Hi,
So what we need is essentially pressurized/compressed air, regulated down to certain level and then pass through an oil filter, and then through water (maintained at certain temp) to humidify it.
Am I right?
Since it goes through a water bubbler, wouldn’t that catch the oil contamination?
We have an oxygen concentrator for our son and spare oxygen cylinders if the power goes out or for transport. Before insurance approved it, an EMT friend actually made the suggestion that we buy the medical grade equipment but fill with welding oxygen. As long as you filter when filling to grab any contaminants from inside the welding storage container you should be good. Passing the O2 through a bubbler helps as well, the water works as a secondary filter. Emergency situations only of course.
Would bubbling the oxygen through an airstone and then through water not filter as well as humidify the air needed for this type of ventilator anyway?
I worked at Swedish air gas producer AGA (now part of german group Linde) and I can assure you there is no difference, at least in Europe. It is just too expensive to have different processes for medical and technical gases and the only difference is that medical oxygen is sold with a certificate saying it is medical grade, and the other isn’t. Just a way to hike prices and revenue.
No there’s no difference at all it’s just the grade of purity testing otherwise it’s 99.99% O2 in “welding” oxygen
The only major difference to consider is the quality. Welding gas CYLINDERS are held to a lower standard of cleanliness. As such they OFTEN HAVE OILS in them from industrial sites. The actual compressors used to fill the tanks can produce the same amount of O2 at concentration.
Perhaps consider dive shops and fire departments that also have compressors.
The difference between the four various oxygen grades, (Aviation, Medical, Welding and Research) is not in the quality of the oxygen but rather, the custody chain of the tanks. … The oxygen can be considered medical grade because you started with a clean tank having no contaminants.
I’m no doctor but i play one on tv– i would think that even mechanical ingress of air has some positive effect compared to the control– at least for all but the most critical cases of respiratory distress
I don’t even play a doctor on TV, but I’m kind of a clown and have blown up a few balloons and think that egress is the part that keeps things from popping
Can fish aquarium materials work?
Joey, is that you?
Doctor Who?…. sorry i couldn’t help myself
lol
I worked on a project related to transfusion related acute lung injury back in 2004, and I recall that it is possible for the ventilation itself to cause injury if not done properly. Unfortunately I was two years out of university and working on electronic monitoring of patients undergoing transfusion, not proper use of the ventilator, so memory is very fuzzy. See below for example. I don’t understand what low tidal volume etc mean. https://journals.lww.com/ejanaesthesiology/fulltext/2008/02000/optimal_ventilator_settings_in_acute_lung_injury.1.aspx
tidal volume is the volume of air in each breath
They did a study and found that lower pressure was actually safer for patients. The normal volumes pumped into patients lungs can actually stretch the lungs out and cause problems. THis article shows that lower volume / less intensity of air is safer.
https://www.nejm.org/doi/full/10.1056/NEJM200005043421801
👅Thanks and…keep on rockin’
Pure oxygen is toxic.
https://en.wikipedia.org/wiki/Oxygen_toxicity
On the Gemeni astronauts got away with it at low pressure for few weeks. At surface pressure I think you get a day or two. And under pressure (diving) you don’t get away with it for long at all!
Basically the oxygen as well as messing up the gradients that means your lungs work to exchange gases literally oxidizes the molecules in your lungs leading to oedema – and acute respiratory distress ARDS precisely the problem we want the oxygen to treat.
So given we are treating ARDS (which is really what SARS means) we don’t want to risk any lung damage that would worsen it.
I think a venturi system would work but I’m no intensivist.
i am a diving professional in saturation and commercial diving as well as a diving medical technician. i can ttell you right now that breathing 100%O2 is fine for long periods as long as you are not below 20 meters of seawater or doing it for longer than a few days. but we are not talking about 100% O2. we are talking about adding 100% O2 to regular air.
I see comments from divers re O2 but also wonder about a conversation of diving regulators to respirators. Just an uneducated idea.
Indeed the flow rate is maybe 20-70l/min and somewhere between 30-100% oxygen. That’s a lot of oxygen you need to add.
Given the choice between 21% Oxygen (naturally occurring) and (say) 50% Oxygen mix, wouldn’t 50% be clinically preferred? Molecular weight of O2 is 32, Nitrogen is 28. Could a rotating separator provide a lower quality, but 100% available source of O2? ex: Spin up a 12″ diameter cylinder 3″ deep and the heavier Oxygen would gravitate to the outer wall. lighter N2 would be found -more- towards the middle? Not looking for high purity, but am looking for something to plug in that would just work.
Unfortunately, such a small system might actually produce trace volumes of oxygen, but not at nearly the flow rate required. The abstract of this article gives you an idea of the technical demands of gas separations centrifuge systems. http://www.mate.tue.nl/mate/pdfs/5250.pdf
Why is this amount required, in the Navy we used the thumbrule of 1scf of o2 per HR per human on board for survivability calculations.
Your calculation is for humans who are healthy, their lungs working at 100%. And ‘survivable’ means some might still struggle.
We want to build something that helps very ill people, with compromised lungs.
An oxygen generator using a hollow fiber membrane could supply these rates. Basically hook an air compressor up to the inlet and there’s an oxygen outlet and a waste gas outlet.
https://www.generon.com/product/membrane-oxygen-generator/
I’ve done this and it works . A standard nitrogen separation membrane filter can produce up to about 45% O2 if you vent the N2 and use the bypass flow as the effluent. It can produce a very high flow rate. These are the types of membranes used in mechanics shops for filling tires and for nitrogen blanketing in industrial applications. The bypass flow rate is almost as high as the effluent flow rate. All you need is an oil-free compressor, good pre filters and an appropriately sized nitrogen separation membrane.
Hi, curious @ChrisHruska where did you get your membrane from? Really interested to try this for an oxygen generation system. Thanks!
Electrolysis could produce pure enough oxygen that was pre-humidified. Bad for storing but that could possibly be suitable for immediate use. Can anyone weigh in on this?
This quora response might shed some light: https://www.quora.com/How-much-volt-needed-to-split-one-litre-of-water-into-hydrogen-and-oxygen-in-1-second/answer/Tom-Nathe?ch=10&share=f6280cda&srid=pGoo
What about the proton exchange membrane technology they use in H2 production for fuel cells? Or Hydrogen production devices which produce O2 as a byproduct as well?
You can also hack a microwave transformer by rewinding one side with a larger gage wire with only one or two loops and rectifying the output for dc output. This is how people make induction heater coils which require a tremendous amount of amperage, but not voltage.
The gist seems to be: the voltage needed is about 1.4V, the efficiency increases with warbler water. Commercial systems run at 80 – 90°C. You need high currents. (4 – 6 kA ˣ m-2)
Could maybe take a play out of the old dynomotor book and make a low voltage high current faraday dynamo driven by a utility AC motor. …. because are you gonna get many high current MOSFETs out of China at the moment?
I am wondering if a larger unit can be built to do most of the functions of the ventilator. The supply and exhaust for each patient could be controlled by a secondary pump that varies the oxygen and humidity. Similar to the main trunk of a furnace feeding separate ducts in a home; There could be a main pump that brings in fresh air and distributes it to different areas.
Other replies are saying they need 20-70L of oxygen per minute, so at 22.4L per mole let’s just go with 2 moles (44.8 liters) of oxygen per minute, and water electrolysis takes 237 kJ/mol. So, 2mol/minute * 237kJ/mol * 1minute/60 seconds = 7.9kJ/second = 7900 watts. Electrolysis requires 1.23V so that’s 6422 amps assuming ideal conversion.
In the real world there will be efficiency loss, here’s a commercial 10kW system that quotes 1000L per hour (16.6L/min), in the end you’d probably need 30kW or more per patient.
https://www.fuelcellstore.com/water-electrolysis-system-10kw
I just made a calculation on this: you need 26,802 Ah to produce 22,414/4 liters (4 Faraday per mole). In other words electrolysis will give you 0,21 Liters of oxygen for each Ah you pass through the electrochemical cell. Assuming that you want to increase natural oxygen from 21 %Vol (air) up to 32 % and assuming further that you breathe 10 times per minute you need 3,3 Liters of electrochemically generated oxygen. Dividing 3,3 liters per minute by o,21 liters per Ah results in 942 A (dont forget to multiply with 60 for min/h) which is much higher than any current output of usual voltage supplies. Assuming that a self build electrolysis cell will not likely work with less than 5 Volt, you end up with roughly 5 kW , which also exceeds what you usually have in your house .
If you are more experienced with the medical side of this, ( I am just a electrochemist) you may play a little bit with these numbers, but the result is the same.
kind regards from Germany
Wolfgang
In a severe shortage you might want to consider aviation oxygen sources. The pandemic appears to be drastically reducing commercial airline flights and their subsequent need for oxygen. This oxygen is designed for human consumption.
Not a bad idea! I can see the airliners willing to cut a deal if they thought they could find a way to save their companies by doing that..
But following the same train of thought: What about emergency oxygen candles? A bit archaic, a bit exothermic, but relatively cheap. Assuming we could buy the materials in bulk, set up a reaction vessel outside (something drip-controllable, like those old acetylene lamps), and pipe that through your filters and compress into tanks or low-pressure gas bags. (a more ’round-the-barn idea, i know, but might be better suited for a more remote area? or if there’s a bad 02 shortage or something…)
Great thinking Norm!
Could you use aircraft as temporary hospitals?
Maybe not for critical care where the patients need pressurised ventilation, but for the developing cases
Pressurize the cabin with oxygen enriched air or use the existing masks and oxygen distribution system already on board. We have airports in every city with great road access.
Alternatively, could the aircraft builders (who have shut down their production lines) continue to build the oxygen distribution systems, but to intall in hospitals – it might be a ward-scale solution instead of a 1-patient solution.
I really like this idea. I am sure airlines are looking for revenue streams right about now, and an airplane seems like a great containment and treatment facility. Rig them up and fly them where they are needed most.
Norm, is the aviation oxygen used only for pilots? I thought the emergency oxygen that drops down for passengers was generated by a chemical reaction endothermic, as mentioned in an earlier comment? These units were being flown as extra freight, and caught fire. This is what caused the crash in the Florida Everglades. The bodies couldn’t be recovered because the alligators ate them.
I understand you can buy med grade O2 from companies like AIRGAS in tanks and have them dropped off…simple to plumb into the system…large tanks…they do it for dive gas as well…produce it in quantity, and deliver it around the country everyday.
What about diving tanks. Are the oxygen for diving perhaps an other posibility to use for the supply of oxigen? Diving is mostly recreational so im sure they can stop diving for a while to save lives
Yes, O2 supplies are bound to be stretched, but other ‘non-medical’ sources of O2 (eg welding O2) are virtually indistinguishable, the main difference is in the tanks and chain of custody – medical O2 is tracked, other sources are not.
In many cases, insufflation of air is better than nothing – even room air – particularly where respiratory distress is exacerbated by a build-up of exhaled CO2 in the respiratory dead space, which can be flushed non-invasively using a high-flow nasal cannula.
increase inlet psi and install regulators on outlet of all recipients
It seems to me that if anything is going to be done at this level and the required scale , you need to pick a the best easiest technology and start breaking out source parts and production.
What type of the device would help? Only a ventilator? The device described doesn’t help? Thanks
Is it really sufficiant to provide a constant flow, but not to mimic inhale / exhale? Thought about this today in the morning and would be really glad to help! Heating Water to 40C seems doable. Pushing constant flowrate through the water also is no problem.
Is there a need for something like an pressure valve?
Could the exhaled / contaminated air be fed through an desinfectand or even boiling water if n95 masks are not available?
Lots of stuff would kill it. Bleach, Disinfectant, 70%+ alcohol
How about UV light? WOuld that “neutralize” the virii? Lets keep our healthcare workers from having to clean up globs of Viruses.
UV-C, yes. But for 30 minutes, from what I know.
UV light would be a great option if it can be reliable for a flow-rate of exhaust air we are talking about.
Hot water sounds like an excellent idea too. I heard the current virus cant survive over 27-degrees Centigrade – but I should qualify that that is third-hand information and would need checking. Therefore the water may not need to be very hot
There’s some research on UV here: https://rdcu.be/b27p8 on using it in a more ambient way, but I guess it could be used intensely within a closed container in this application.
(Not an expert)
I feel like heat and fuel sources are to be avoided if it’s oxygen enriched air that’s being exhaled.
UV-C should be used in the intake humidifing water too to ensure the water is sterile.
Nasal NIV is not closed so the person continues to ventilate but high concentration is delivered into the lungs to aid gas exchange.
It won’t be used ventilation is needed.
Again I’m not intensivist
Creates aerosols. All CoV patients are to be ventilated via ET tube, mostly because of ARDS and the complexities of gas exchange and lung compliance in these patients and partially to protect staff. Nasal high flow is available and very cheap compared to a invasive ventilator.
When it gets to the stage that most people are infected, making aerosols of the COVID-19 virus isn’t as much of a concern.
For those already infected or recovered, breathing in a few of the same virus won’t make much difference.
I’m not much use at building ventilators, but as to masks, I’ve done a lot of investigation and come up with a reusable design in fabric which is freely available and finely woven enough that it prevents bacteria, viruses and dust from passing through. The item could be soaked in bleach (which kills all germs, such as Jik ) and washed for wearing. I’ve made several samples and would be keen to share the patterns and links to articles describing the benefits of the fabric, anyone could make these masks, and each person only needs 2, 1 to sterilize and 1 to wear.
This is something I am very interested in. I’ve seen some designs, but your’s could better, and I would love to hear about it more.
hi Susan. Great idea. good thinking. Please share your patterns via internet.
Regard’s,
jt
Please put free patterns up on the internet. There are a few available patterns (and they don’t sound as good as what you are describing) but the instructions are in Chinese.
This is something lots and lots of retired nurses and others would LOVE to produce for our currently working sisters and brothers in arms currently working in hospital. Please share your design here!
I for one am interested. My daughter is a veterinarian and they’ve been having to make their own masks. We’ve got a couple of sewing machines and a handful of servers here
Please share directions to make this mask. My daughters and niece are healthcare workers. They need this!
I have experience in designing negative air pressure containment areas for asbestos abatement. How is the exhaust air for the negative pressure containment area disposed of. In abatement, To create negative pressure, you have to keep removing the air from the inside of a space so that nothing can go out, but that air has to go somewhere, usually through fans and HEPA filters. Disinfecting patient exhalation may be easy to disinfect, but what about the room air?
I was under the impression that HEPA filters would be suitable to filter out most viruses but not all. Maybe if you were to ionize the air prior to the filter though and then have a mesh prior to your HEPA filter that’s positively charged. Like this study https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4477231/
Just a thought–UV (XEnON) lamp on the backside/exhaust side of the HEPA filter and then pass the treated air through a secondary filter…want to get fancy…line passage between first filter/Xenon lamp and 2nd filter stage with silver so you don’t get short term build up of virus on surface.
Hi Susan, I’m keen to see designs too! Sounds great and I could produce these for people if I can get the material.
Sounds great Susan, please let me know where you are posting the information. Thanks
I am working on a bit – I found a filtering material that is readily available and is designed to stop virus transmittal along with smoke and otherwise. Should be able to make a mask with a hot clue gun and some fabric, a house air cleaning system with a box fan and some tape, or even a canister breather with a soda bottle and a hot glue gun. Doing a bit more research on it.
I would love to have your pattern: A family member has been put on alert that their hospital is being set up to take NYC overload cases. They do NOT have enough masks, and my wife and I are setting up a (Free) cottage industry to make fabric masks. Please email me at tom@baccei.com Thanks You!
Please post your design in some way. Many of us could use it.
I am interested in how you are making masks. Please share patterns and sources
Can you make one of your masks? even only as proof of concept at this point is valuable? Doing nothing is far worse then doing something and failing!!!!!
I’m interested.
There are liquids like oils with much higher boiling points and viscosity than water, perhaps bubbling the exiting gasses through these liquids at high temperature could kill the virus. Basically deep fry the returning air.
Copper is shown to kill coronavirus, a copper mesh filter could be manufactured, multi-layered for maximum efficiency. Increase the chances of collision between the airborn coronavirus and copper surfaces. The copper ions destroy the coronavirus outer shell. I am not certain about the reaction time (virus to copper contact time) and ideal temperature for optimal results. Heating the copper mesh with electrical resistance may increase the efficiency. Hot dry air and multiple collisions of virus to copper mesh surface. Bill Keevil research in the US on coronavirus and copper.
Might be as easy as running voltage to a copper mesh contained in a stainless steel housing coupled to the ventilator.
Could regular liquid heat transfers made from copper to be transformed to use as a exhale filters then?
Hey this sounds interesting is there a possibility to charge the virus statically and improve the collision chance with the surface of the copper in order to minimize the travel distance of the virus through a mesh?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4477231/ they did a study on it. It’s definitely possible.
I like the sound of this, keep up the good thinking! Wonder also whether a nanosilver mesh or fabric like the bacteriocide used on socks would work?, maybe multiple fine layers.
Electrostatic attraction?
“Copper is shown to kill coronavirus” Please provide a reference. I do NOT believe this is true. This says 24 hrs on copper or carboard and 72hrs on Stainless/plastic – https://www.caltech.edu/about/news/tip-iceberg-virologist-david-ho-bs-74-speaks-about-covid-19
Please be careful about posting postulations w/o a disclaimer.
I’ve seen 2 others, one said 40 mins and the other said 4 hours. However, relative persistence times on other material seem to be equivalent, so I guess it’s how big a “drop” it is you put on there, local humidity and other factors.
Use a f**cking hairdryer to suck away contaminated air. If it’s not hot enough then choose one from the hardware store (those 650°C blowers used to remove paint). They are cheap. The Hairdryer can also be improved by adding a long insulated pipe at the exaust which will give the hot air more time to destroy the virus. (Viruses cannot be killed as they are nothing living, neither Corona nor Stuxnet.)
Anyways, I think disposing contaminated air is not the main problem.
What if you bubble the air through a liquid containing copper ions?
Would this kill the virus?
Could a CPAP machine be modified? They warm and humidify air, just the way it’s introduced to the patient is different, could a nasal cannula adapter be made to fit the end of the hose where the mask would usually go on? (Sure it’s far from perfect but it’s more perfect than nothing.)
I don’t think so. I have a CPAP. It’s nothing like a ventilator at all. It just raises the pressure of the incoming air a bit (and not all that much). You still have to breathe yourself.
PS: warming and humidification is an option on most CPAPs by the way – I had it but I got rid of it because I felt the walls closing in on me with that watery air. Also the whole process of cleaning and decontaminating it is a PITA (after all bacteria just love the warm temperatures it uses).
During the winter the cold air dries out my nose a bit and causes skin cracks but I smear some vaseline into it with a Q-tip to protect the skin and that works fine.
Why not use one of these to centrally supply air to several ventilators?
https://www.govplanet.com/jsp/s/item/2769192?kwtag=p13n-SL&h=
I don’t know about hospitals in Your country but those i saw in my have central oxygen, vacum and some other valve i don’t remember. There are pipings through whole building to central pump station. I doubnt hospuitals in 3rd world are built this way, we in developed countries will probably have enough equipment but i’m thinking abiout folks in Africa or refugees in Syria they are fucked.
I disagree. I believe a CPAP absolutely can be modified to inhale/exhale with a few mechanical and sensor hacks.
i’m with you. i have both a cpap and an apap, converting a black light panel into 200W UC-c.
3D print a spacer to fit between the CPAP mask and the hose with a fitting for a O2 line. In an emergency, make a small slit in the hose near the mask, insert the O2 line, and seal with duct tape.
I don’t think you need to do anything else.
If you put it in a negative pressure tent, the tent has a HEPA filter on the exhaust fan, reducing the aerosolized virus threat.
My resmed airsense 10 and many other CPAP have an “air ramp”to gently increase pressure to allow people to get to sleep.
All you have to do is hack the software for the “air ramp “ to simulate breathing . That I put in a continuous loop. Also you probably don’t need super high O2. concentrations for EVERY person who needs a ventilator so either adding O2 after the CPAP WATER STAGE or if it was a low enough concentration of oxygen, you could fill a large Industrial garbage bag partially with oxygen and then put the CPAP machine inside that. That would probably be have to be less than 25%. 02. Since Air has about 20% oxygen he would end up with a concentration probably around 45%. Failing that, you could probably tape off some closet and fill that closet with some O2. Are using the garbage bags so you know you wouldn’t overdo it. Toss the CPAP in there and you would get a gradient of decreasing oxygen over time, but every so often you could introduce another garbage bag of pure O2 into the large closet.
Yes, they are set to reduce pressure during exhalation. The result with a plain cpap feels like good air in bad air out. The weight of chest components, ribs muscke skin etc passively promotes outflow. There are bipaps that are infact complex and computer regulated ventilators. Your pulmonolgist or sleep specialists should be able to help. They should also be thinking out of the norms for solutions. Cpap/bipap companies include Apria and Norco. See if you can contact their engineers and respiratoty therapists. All these ideas I am reading especially ifcombined could save a lot of lives.
One option for decontaminating warm wet environments is to simply have two of all the parts of the system which are warm and wet, swap them over every 12 hours, and put the not-in-use one into boiling water for 10 minutes.
I was thinking of combining a CPAP machine with a continuous flow oxygen concentration. If they are to be used at home, perhaps the contamination is not too big a deal. What flow rates do ventilators have? What flow rates do CPAPs have? 3 liters a minute? Higher?
yes. bergamo ED have had success with CPAP hoods
CPAP machines are currently in use in hospital ICU’s as a precursor to intubation and mechanical ventilation of patients. Supplemental oxygen is added to a side port of the machine and the person gets added oomph to force oxygen past swollen and thickened lung tissues into the blood.
Wouldn’t that just cause the same problem as a CPAP and just increase transmission of the virus? The only difference would be the size of the hole and the amount of re-breathing. (CPAPs rely on rebreathing a portion of the volume of air and a calibrated leak to restrict pressure and amount of re-breathing.)
Wouldn’t a jet ventilator be better?
yes, you need to conatin the breath out and flow it through a UV-c field, of bubble through a liquid
That’s cool, is a manual resuscitator with… mechanical hands to operate it
https://en.wikipedia.org/wiki/Bag_valve_mask
link doesn’t open
What about using SCUBA re-breather technology to scrub the air and make the system closed loop while injecting O2?
was thinking the same thing… older DIY rigs look to be rather easy to make, and I would think the sodium hydroxide scrubbing the CO2 would have an added benefit of possibly killing any virus that was exhaled (at least getting it clean). Should be rather easy to add some activated charcoal for additional filtering.
only thing I’d worry about might be adding a humidifier due to the whole “Contact with water causes violent frothing and spattering” aspect of NAOH (Lye).
This checks off most boxes, and in an emergency situation, this can be easily built and serve as a solid platform to be built upon to achieve the required goals.
– simple to build and reasonably cheap for consumables
– closed circuit air flow to prevent/reduce chances of passing on infection
– relatively low cost
– easy to modify/adapt/clean
– easy to add to existing infrastructure or use in field
– portable
– reasonably low tech with options to easily add capability
Here’s an example of an early DIY rebreather that should be easy to build.
https://www.youtube.com/watch?v=xVNsE405UWI
I mean it gives one great hope when they describe one machine and show a picture of another, yes I will trust this to be nothing but entertainment, how long before it requires a PI to control a 16×2 LCD?
I have designed & mfged any number of naso-gastric feeding tubes, as well as a number of other GI related devices. I believe I could readily design/copy a high flow nasal cannula.
CPAP machines?
So, what is indeed needed for a severe SARS-Cor-19 infection?
there is a good critical care reference on various vent modalities in COVID that might be very helpful. Would consider reaching out to the author if viable prototypes are being designed EMCrit.org/IBCC
If we assume all elective surgeries are put off for the duration of the emergency, how many machines used for mechanical ventilation during surgery can be repurposed?
Average length of stay for elective patients is about 4 days, of which (say) 3 are post operative and 1 or 2 intensive/High care. Length of stay for a 70 y.o. patient with viral lung issues and on ventilation is about 16-20 days. This equates to about a 10 to one equivelence. i.e. 10 electives cancelled for each Emergency case.
I would think it’s worse, I’d hope someone recovering from surgery doesn’t need to be ventilated much longer than they’re in the operating room…
In Italy they are not doing surgery, they’ve re-purposed the operating rooms for ICU patients.
https://www.youtube.com/watch?v=zEFfpGsdUXM
Yeah, I was a plumber. The portable O2 machines could concentrate the oxygen, steam from sterilizers could be piped to warm/humidify air, cannulas and the plastic pipes are everywhere, but we would likely need for mfrs to ramp up construction of those and we would need more generators.
So the patients are able to breathe ok, but the air just needs a much higher concentration of O2? They don’t need to be intubated? This is a lower respiratory disease, lots of fluids, iirc. Enough presssure is really generated with a cannula?
I am a product developer with loads of experience in software and hardware. I also may have access to a large pool of engineers.
I work in business development in a small manufacturing area of Western NY. We have a ton of metal benders and precision manufacturers. If there were a way to develop a simple-to-build design, with a basic interface, I feel confident we have the bench to help build these machines quickly.
So did you see the post that included the link to the MIT 2010 design. If not I can send it to you. I am Richard@worldhelm.co.uk
Hi, interested in talking with you about a project I am working on. Portable ventilator unit, bill2resist@gmail.com
Thanks
Bill Rasmussen
I just found this amazing site today and ifbyou are still looking, very interested. Please see my comment on CPAP.
Nancy Lord, MD
USPTO reg no 45462
Haven’t seen any activity here for a while. I don’t know if Bill is getting notifications.
You can consult with a 3d printing company for rapid prototyping a simple and affective device that can be quickly manufactured on a large scale. This would save many lives and could be a stop gap solution until the patient is put on a conventional ventilator.
Hey Simon,
Our platform has access towards 450 3D print location in more than 40 countries that can supply 1200+ 3D printed materials. The only problem is that we don’t have the designs. Also I made a list with critical parts (UK government list) that is necessary against corona:
List of critical parts – https://docs.google.com/spreadsheets/d/1bNjj23e5jFHIf-2XRq_RhuYsdASIoW4t5FKtAd2EiVM/edit?usp=sharing
3D print platform – http://www.quote.beamler.com
Article about valves that are 3D printed in Italy. Currently 10 patience are using these: https://www.beamler.com/3dprinting-coronavirus-flatten-the-curve-covid19/
Hey Willem-Jan,
Good that you want to help out! This page contains more recent info + discord channels for 3D printer owners. https://3dprintingindustry.com/news/3d-printing-community-responds-to-covid-19-and-coronavirus-resources-169143/
Are cuirass ventilators suitable for this virus? Similar to the iron lung used to treat polio. Obviously these would be the easiest to manufacture.
Short answer used to be NO, They need to be molded to the individual, a plaster cast is made of the chest, then a fiberglass shell is made from that. There may have been improvements from when I worked with them but as far as I know not much has been done.
If fitting is a concern, then what about an iron lung? (Yeah, they look terrible, but it’s not a time to be picky about aesthetics.)
Iron lungs would work but…you need to find them, then you need to replace ALL of the gaskets and rubber seals…If you can find them. Rubber from the 50s has not lasted well.
Regarding the negative pressure Iron Lung – or the emergency Both Respirator built in 24 hours in an emergency, would it work as an emergency measure. There is no intubation needed, and patients do not need sedation (which in itself can be dangerous).
As for the Hack Community – years ago I designed a shop vac powered trash compactor after our City decided they would pick up only 1 approved container. I used one of those 96 Gal large Rubbermaid garbage cans, had a cut plywood with a rubber door seal to seal it on vaccum to the container top (it is flat). I then cut a round piston plywood insert – maybe 2 feet diameter with a cylindrical rubber bladder with a vulcanized seam. All sealed to the Plywood with silicon rubber. I left a vaccum attachment to hook the shop vac. These cans are air tight and would work well – the thicker ones. It worked great.
As an emergency measure, one could put a seat or chair inside and make an equilevent plywood to trash can seal with a hole for a neck??? What pressures are needed for such ventilators. I would put my 92 year old mother gasping for air in one when there are none available for her in hospital settings?
I just want to know will the negative pressure ventilators – Iron Lung work at and at what frequency. They saved a lot pf Polio victims survive for 2 weeks needed for the diphrams to work again – hopefully.
Obviously I’m not sure of the specific design requirements, but there must be loads of model makers, prop makers, special effects make-up artists etc who are now out of work and could easily do much of this. I’ve done similar work many times in the production of SFX prosthetics, moulds, masks, armour etc… There are fast drying resins, but would still take a fair few hours per unit – if each is bespoke. Obviously could be mass produced quickly in a range of sizes if that works.
Boiling the virus in water sounds legit but subsidence time of a water droplet inside hot water would not be thorough enough. What about a small UV light similar to those in backpacker water purifiers mounted to the exhalation exhaust would make a PAP machine usable and sterilize exhaled air. As long as the light was shielded the patient wouldn’t be subjected to the UV.
My idea takes a single piston design which uses a simple electric motor to create the strokes needed for ventilation. Simple hand dials can regulate stroke speed and O2 volume, and using a warmed water vessel for the O2 to bubble through. This device could probably be built for less than $200 and be assembled in less than 8 hours. And the as the “exhaust” stroke delivers O2, the “intake” stroke can pull the exhaled air out using one way valves to prevent the airs from mixing.
The. Piston stroke volumewould be calculated to be normal breathing volume I have seen it on a website chart something like 7 cc per kilo body weight. Here is a plan from 1950s http://blog.modernmechanix.com/diy-iron-lung/ .I posted somewhere on this site some info and research that I have done but cant find it now
https://en.m.wikipedia.org/wiki/Lung_volumes
Short of a full blown respirator, is there something of use that could be pulled together with a concentrator (or multiple)? would 3D printing of a mask help, perhaps with a 3d photo scan of the patient’s mouth?
Hey Tom,
I looked into 3D printing a mask. It is quite difficult because of the filters. See this link of a self made mask: https://www.opensourcemask.com/en/
Hey Albin,
with the shortages in ventilator we’re facing, it would be great if you could describe what exactly would be needed from a system like this?
i.e.: Ideal vs minimal system
Ideal: o2 connection, o2 filter, intubation connection, humidifiers, heating, controllable pressure, flow etc.
Minimal: is it any use without o2? humidifier and heating seem easy to implement, could one make fixed flow and pressure? what would that volume be?
Thanks
the flow would need to be 150 lpm for open system..see BiPAP. and for closed system up to 100 lpm but probably more like avg of 60 lpm. without the flow patients may become air hungry.
As for pressures, you would need pressure limits of 40 to 45 cmH2O. lung damage occurs at about 32cmH2O.
I think a mode of ventilation that would be safe and easier to construct would be airway pressure releasr ventilation. a constant pressure applied with timed releases of 0.6 to 1.0 seconds. APRV or bi-level.
this is the safest mode of ventilation I know of. you just need a flow generator, a pressure limiting devive and a way to time releases, no peep valve needed for this mode.
See the Montreal Challenge they provide full spec`s
Does the unit simply supply oxygen rich air at a predefined rate?
Or does it need respirator control mechanics?
In the 1950s and 60s fire depts began carrying ventilators. That was prior to formal EMS trained technicians. They eventually withdrew the units as ff working them were doing more harm to patients prior to reaching hospitals. Things like over pressurizing injured lungs. So you gotta be careful proposing cheapie alternative units run by who knows what.
I think you may have been thinking of the Demand Valves, A round hand held device with a button on top. Yes they were terrible. No pressure relief or none in the safe human lung range. connected directly to a cylinder.
Double or triple percolator for water humidity control
And for oxygen I do not know about its solubility and technical matter
would a Both Respirator work (kind of iron lung) https://en.wikipedia.org/wiki/Both_respirator
Apparently you build them out of plywood?
It sounds like an awesome idea. I prefer this one because it is cheaper and simpler to make.
How durable is that pool of water (kept at the ideal temperature for whatever is in there, to grow)? Does it not become a source of infection itselft?
Could you please look into https://www.agvahealthcare.com/models
They claim to be worlds cheapest ventilator makers.
I wonder if a Cpap machine could be hacked to facilitate this?
What if you just use a standard respirator like cpap but reroute the exhaust into a treatment system (uv, ozone, dessicant, the works). This way it could be retrofitted onto existing respirators, you just need a new mask and the attachment. A concern is if the face mask seals could be leak-resistant enough and if the air treatment requires too many actions, how cheap/easily it could be made.
I’ve been wondering if a scuba closed circuit rebreather can be reconfigured as a replacement source?
I feel as though creating this device would be simple enough, but we also need it to clear regulations so people trust the device. Any one have any thoughts on how to make the device ISO compliant? I just don’t see this device actually being used unless it meets some sort of safety requirements.
So despite media verbiage, which device is the one that is needed? A cannula or a ventilator?
There are literally millions of oil free air compressors in the world. They are used by home owners and contractors for construction. How can they be utilized in a ventilator package?
Medical Device Designer here.
Would I be simplifying this too much by saying this is a moist air pump.
you need a constant base pressure of at least 18 cm H20 and ventilations of about 330 mL
What i see in the news: people that have difficulties with breathing at first need a cannula but later almost always need a proper ventilator which is more difficult to get. So building an open source ventilator is probably most important
Albin are you on the Slack? You should review the proposals!
Very important project. Ive made a github project for it: https://github.com/rune1234/DIY-respirator
If the device described in this post is “not a ventilator” is it actually what is needed to save lives during this crisis? I think the initiative to build an open sourced ventilator is magnificent, but don’t want people directing time and energy trying to solve the problem by building the wrong device. Any thoughts in your medical opinion?
For the nasal cannula, maybe use a 12 volt portable air pump (normally used to inflate tires) with the nozzle cut from an inter-tube. Cut the end of a bike inter-tube nozzle to glue onto the end of the 2L bottle cap to seal. This can then be connected to the 12 volt portable air pump. Will have to find a way to have the bubble gas as input to the air pump. Could also use an aquarium pump maybe too.
I have been thinking of cutting the top off of a 2 liter plastic bottle, drill small holes in the end cap and insert cloth at the end as a filter for a bottle mask so people can protect themselves where masks are not available.
I am not sure what your wanting to do, vents are different from CPAP, and mask are a lot different, first issue with mask is if they can’t filter virus then not much use.
Always one to be contrary and think outside the box here. Is there an effective way to filter out the “aerosolized” exhaling that would allow for CPAPs to be used. Seems like everyone I know has a CPAP. Is it reasonable to say use a CPAP as a method of last resort in a situation where you had no caregiver nor anyone else around to be contaminated? Would using the fabric from a high quality home Heat & Air filter be an acceptable tent to place over a patients face in hopes it would ground the exhaled virus? I’m not medically educated so I’m ready to have all these simple ideas shot down. Also, Albin, are you saying the high flow nasal cannula is not what we need or is it an acceptable substitute?
Hello, I am looking at a small constant flow device fitting on the end of tube, pressure regulated , rate based on flow rate and compliance, there is a possibility we can use LMA or regular intubation,
Also looking to use perflurocarbon , liquid breathing, for better vent performance.
It has been evaluated by other MD so looking for a medical advisor for the project
Could you post an image of a ventilator .
There was a study that shows that one ventilator can be used with up to 4 patients as an emergency MD demonstrates here https://www.youtube.com/watch?v=uClq978oohY
She said it has been successfully used on people during the Las Vegas shooting tragedy, when a former student remembered the study on this and was able to use this to save lives despite the shortage of ventilators during the emergency.
It can and should only be used in dire circumstances, but just look just how dire the situation in Italy is. The hospitals got overwhelmed by the sheer numbers of new cases, the doctors find themselves making difficult choices over who to treat with ventilators and who to send home.
For me hooking up multiple patients to one ventilator looks far more feasible (and faster!) than making DIY ventilators. Let’s leave DIY hacks for less complicated stuff that can still help such as face masks or face shields which are relatively easy to make even at home e.g https://hellosewing.com/homemade-plastic-face-shield/ and https://hellosewing.com/face-mask-sewing-pattern/
Ventilators are invasive devices and its not just the ventilator – you need a skilled HCP to manage the ventilator and the patient. Certainly not something to be done at home
Hi Helen,
Great to see a touch of rational thinking in this thread …
We SHOULD NOT BE TRYING TO MAKE A VENTILATOR.
We can’t make a ventilator using bits and pieces from the hardware store.
It’s not scaleable, and you need a HCW to operate them.
How can you hand-build 30,000 ventilators, deliver, deploy and support them, and train people to operate and maintain them in 100 different countries – all in a couple of weeks ?
ITS NOT POSSIBLE
We need to find ways to keep people OFF ventilators, using non-invasive therapies that don’t contaminate the workplace – which would INFECT HEALTHCARE WORKERS and INCREASE FATALITIES.
Yes – DIY hacks have a place where it comes to making something simple – not ventilators.
Lets go back to the original brief – NON-INVASIVE therapies.
See my other posts – we need to support supply chains for people who ALREADY KNOW how to make ventilators – and masks – and stop hoarding masks and groceries.
“We SHOULD NOT BE TRYING TO MAKE A VENTILATOR” – I agree with this from a pragmatic perspective, however I disagree that we should leave ventilator manufacturing to those who already know how to make ventilators for the exact same pragmatism. It will take 90 days MINIMUM for industry to start churning out ventilators and even longer to manufacture the required numbers. We don’t have that kind of time.
So what CAN we do? We can start by putting our heads together and creating a ‘Ventilator Performance Specification’ which documents WHAT such a device should do rather than specifying the details of HOW the device should do it. The type of document I am referring to is common both in fielding software systems as well as FDA and DoD system.
In the software industry, there is something called ‘Verification and Validation’ which can be understood as the difference between these two questions:
1) Are we building the RIGHT product? (will our DESIGN satisfy the customers requirements)
2) Are we building THE PRODUCT right? (does our PRODUCT match our design)
Such systems as the ventilators in short-supply are subject to an overlapping set of requirements held by many, often conflicting stakeholders. Hospital attorneys will tend to take the position of, “let patients die rather than utilize an uncertified device” in order to avoid liability. However a competent med-tech, confident that an uncertified device he is familiar with will function as required to save a patient, would often be willing to accommodate special circumstances IF a path to alleviating liability is provided. The success of any such device relies as much on providing a methodology which allow attorneys, hospital admins and the rest the ability to ‘triage’ by providing policy guidelines to accommodate the special circumstances as it does the technical capabilities of the system in question.
A performance spec serves as a guide for those ranging from small businesses with equivalent tooling to traditional medtech companies such as Medtronics as well as the Makers whom are posting here. It details the stakeholders involved (doctors, med-techs, hospital admins, hospital attorneys etc.) and outlines the various concerns of each actor to provide a high-level understanding of the environment the system will need to accommodate. Such a document specifies requirements in terms of interfaces allowing the individual designer the flexibility to satisfy that requirement while also detailing ways of testing whatever device is created in order to ensure those requirements are satisfied.
A performance spec is typically what the DOD or FDA would provide contractors whom wish to bid on the design and manufacture of a device that would meet the needs of the the customer. Each contractor THEN provides a detailed DESIGN specification that shows what components are connected in what fashion to manufacture a working device.
I believe we should focus our collective efforts in this area in order to provide ‘lift’ for these other technical efforts. Given the amount of people interested in contributing, I also believe suitable devices can be fielded in far LESS time than massive, inflexible manufacturing facilities whom are trying to meet rigid standards which many in the medical industry may be willing to grant special exceptions under the circumstances.
“However a competent med-tech, confident that an uncertified device he is familiar with will function as required to save a patient, would often be willing to accommodate special circumstances”
There are 3 key words here that contradict the rest of the argument …
COMPETANT
There is no point making 30,000 home-made ventilators if they will be used by inadequately trained staff – Ventilation is s a HIGHLY SKILLED art – and often requires sedation and intubation. You cant turn people into ventilation experts by getting them to read instructions out of the box.
CONFIDENT
Medical Device certification requires products to be designed in a Quality-Managed development environment.
THAT is what gives confidence to hospitals and operators.
Would you let someone operate on you without a degree – or do you expect to see a certificate on the wall when you visit a specialist ?
FAMILIAR
How long do you think its takes to become familiar with a new piece of equipment, the accessories that go with it, the effect it has on patient health, and the consequences of getting it wrong – which means you’ve killed someone ?
Does it make a difference when every device operates a bit differently because the’ve been fast-tracked through calibration and certification – or there’s a bug in the software because it’s been designed by someone with no expertise in respiration and hasn’t been rigorously tested ?
Now Im not saying that I wouldn’t make something using a plastic bag and a windscreen wiper motor if it meant saving a life – but that’s different to trying to do it to save a million lives – particularly when you dont have a million HCWs to look after them.
The BIG obstacle is to avoid producing aerosolised virus-laden exhalate – which will infect healthcare workers and case emergency care to collapse – and INCREASE FATALITIES.
Best thing is to support supply chains and routes to market for ventilators made by people who know what they’re doing.
They have ramped production up to100% and are re-purposing designs to meet the need.
https://newsroom.resmed.com/news-releases/news-details/2020/ResMed-Statement-on-COVID-19/default.aspx
” it’s about build devices in QUALITY-MANAGED environments” I am not sure how many Performance Specifications or Test Specifications you have actually authored. I would guess not many.
There are TWO methodologies regarding certification, both recognized by the FDA and DOD.
1) The ‘standard’ process utilized by systems such as medical devices and aircraft. Focus on quality control of the manufacturing processes while employing a ‘Go/No-Go’ minimalist testing program in favor of mass production. (if everything isn’t perfect on an aircraft, it doesn’t fly. period) This process is the default for systems which ARE NOT EVER expected to function under circumstances of degradation.
2) Test-Oriented Product Development which places less emphasis on the quality of manufacturing and instead emphasis rigorous TESTING which qualifies it’s ACTUAL rather than THEORETICAL reliability within a specific tolerance.
Has it ever OCCURED to you that testing as well as self-diagnostic software can also be tailored to ensure any device however it was manufacturered functions ABOVE a specified reliability rating WHILE ON SITE before it is used on patients?
Tell me; what metric provides a HIGHER degree of reliability confidence?
1) Controlling the circumstances under which a device is manufactured and then hoping the HELL the device isn’t damaged in transit to the hospital or during installation?
2) Passing an embedded Test which ensures at slightly higher than acceptable reliability rating ON-SITE, once hooked up and ready to be utilized thereby BYPASSING the risk involved with No. 1?
If you are an engineer, I could excuse the autism…
Hi Shawn,
I’m not sure whether you have any experience in medical devices or respiratory care …
I’m the founder and CEO of a company that designs, develops and commercialises Medical Devices.
I’ve spent 40+ years developing medical devices, including Class III active implantable such as :-
– pacemakers
– implantable defibrillators
– respiration monitors for intensive care
– insulin pumps
– cardiac monitors
– pacemaker test systems
all in a quality-managed development environment consistent with IS0-13485 and a dozen other medical device and software standards.
These are devices that can KILL YOU if they don’t work properly.
So yes – I have authored and worked under my share of Performance Specifications and Test Specifications.
And yes – I understand about software self-testing – I forgot to mention Im a computer scientist with 40+ years experience in this area – including software for implanted devices and for devices to program and test them.
I suppose that qualifies me as having sufficient experience to comment on this topic.
Im guessing you’ve never developed a medical device, otherwise you’d understand the standards govern the design process and risk identification, in addition to the actual product. You cant identify every risk by testing the manufacturing process or the product, and software cannot test everything. How could software test the mechanical reliability of ventilator line – or whether exhaled air from patients contain aerosolised virus – which can infect healthcare workers ??
Some followers of these threads are falling into the trap of specs-manship – ‘I can design a better device than you can’.
Your estimate of ’90 days minimum’ for industry to start churning out ventilators is simply wrong.
People who know what they are doing have already tripled capacity in quality-managed environments with all the appropriate certifications, and have shipped tens of thousands of devices in recent weeks.
Here is just one of them … there at least dozens of others doing this in the USA alone + Europe.
https://newsroom.resmed.com/news-releases/news-details/2020/ResMed-Statement-on-COVID-19/default.aspx
So – in answer to your question “Tell me; what metric provides a HIGHER degree of reliability confidence ?”
The answer is this – certification under the global medical devices regulatory framework.
Now there are emergency exemptions to these standards as you can see here …
https://www.fda.gov/medical-devices/emergency-situations-medical-devices/emergency-use-authorizations
but these apply to the modification of devices that have already been designed and certified **by people who know what they are doing** – and modified for this specific purpose using the same quality-managed processes.
Hackers will never be able to keep pace with existing manufacturers, who have the resources, designs, facilities, processes, trained staff, supply chains and distribution networks to make product at scale and deploy it globally – with the proper metrics for performance, reliability AND confidence – AND TRACEABILITY and SUPPORT NETWORKS.
The real bottleneck in this crisis is NOT VENTILATORS.
It is Personal Protective Equipment for front-line healthcare workers – and having enough HCWs themselves.
We are at risk of not having enough front-line HCWs to deploy and manage the number of machines already being delivered.
If machines are hacked and poorly deployed, they run the risk of infecting HCWs, who then become patients, creating a destructive loop in the front-line, which leads to INCREASED FATALITIES.
We can all make a much bigger difference by modifying our own behaviour to CONTROL SPREAD OF THE DISEASE – focus on hygiene, safe distancing, stop hoarding, care for others in need, and support supply-chains for manufacturers facing input shortages, such as PPE.
Hacking a ventilator is not what we need – and is NOT what this thread was created to do.
“FAMILIAR
How long do you think its takes to become familiar with a new piece of equipment, the accessories that go with it, the effect it has on patient health”
Yes, because you are dealing with proprietary rather than open performance specifications, which was the point of my entire post. All proprietary vendors simply develop Design Specifications and a separate Test Specification which conform to FDA established requirements. If the FDA or DOD, acting as a customer wanted to field a system, they would internally create a Performance Spec which would then be used to conduct a Request of Proposal. The Gov would use their own Performance Spec to drive development of any Testing Specifications to then qualify that new system.
What difference would an OPEN performance specification make?
Ever used Marlin on your 3d printer? Funny how no matter WHAT type of printer you have, you can still compile the same firmware with the same menus and configuration opens regardless of the hardware you are running.
Gee… that sounds like an approach that might be useful in standardizing the interface to a bunch of machines using different hardware yet designed to perform the same function….
Perhaps you might find this video helpful …
https://www.youtube.com/watch?v=7vLPefHYWpY
Why is it necessary to use pure oxygen? Why isn’t just plain air good enough? Is this a liability issue concerning impurities in the air?
And why is it that when we breathe, we don’t need to breathe humidified air in order to not dry out mucus membranes? Is air humidification the only way to prevent mucus membrane from drying out?
http://www.ventilaid.org/
this is the initial phase of the open source project, what do you think about it ?
Wouldn’t a Negative Pressure body shell with oxygen therapy be a more likely ‘open source’ option? Not all cases necessarily require intubation and in fact some studies showed better outcomes and lung recovery.
Is a ventilator a closed loop device or does is vent exhaled air and supply fresh air?
Would a biphasic cuirass ventilator work with most case just assisting them? One might make a wood plenum and pump the air with a piston in a pvc tube powered by stand mixer, aka KitchenAid with accessory attachment port running a crank of adjustable stroke?
Why can’t we modify heavy jets heating / pressurized air bleed from like Boeing’s 737… modify air as needed remove all seats install beds and utilize aircraft for ICU ventilator… an anesthesiologist like yourself could mandate psi needed along with temperatures etc… this isn’t pretty but theoretically it could meet the demand needed on time, space, safety while providing ventilation as needed…. dutchman
I’m honestly not certain whether this suggestion is serious … but the word ‘safety’ should be underlined.
You need *differential* pressure to ventilate a patient.
Unless the signoff ‘Dutchmen’ is an epigram use to express disbelief – as in ‘if that works, Im a Dutchman’.
In England they making simple respirator with open source. The mechanical device is inside a plexiglass box and they push the air with changing pressure in the box, to compress the mechanical device. They designed electronics to run it. I know that readily available programmable devices can be set up to run it. These can be made in a few days. Simple but they work.
I think you might be referring to the OxVent project.
https://oxvent.org/
I cannot see the point of using a compressed air supply to compress an Ambu bag to generate compressed air.
Ambu bags are designed to be used by a highly trained professional who adjust compression depth and timing according to the needs of the patient, in a situation where compressed air is not available.
The idea is not new.
http://www.freepatentsonline.com/20190336713.pdf
There are many similar devices.
https://e-vent.mit.edu/
If you already have a compressed air supply, any advantage the bag offers to limit pressure and volume can be more easily achieved using regulator valves like those in a scuba tank – no electricity needed, and already available.
It cannot assist clinically without a controller and feedback loop to synch with patient needs.
It will never be adopted in clinics.
It cannot scale to meet the need.
Manufacturers of ‘real’ ventilators are scaling up massively and will get *certified* product to market way before a hacked solution could be rolled out. They have certified designs, quality control, a validated supply chain, ability to manufacture at scale, as well as distribution and support networks.
An example
https://newsroom.resmed.com/news-releases/news-details/2020/ResMed-Statement-on-COVID-19/default.aspx
Generating air flow does not solve the problem without a proper connection to the patients.
Where will these projects siurce lines and masks ?
How will they manage virus-laden aerosols that can infect healthcare workers, turning them into patients, causing front-line clinical care to collapse, which will INCREASE FATALITIES ?
If a patient is so sick that they need respiration support, then this is not the answer.
Not this OXVENT but the EXOVENT ::https://www.exovent.info/
What percentage of humidity and O2 saturation at what flow rate are required?
Is there anyway to use an aquarium air pump, 3D printed flow regulator that works like a pressure valve to attain the correct pressure range. i am nobody, but was trying to work out the math for the PEEP, to create a mechanical moving rotary flow restriction that simply hooks up to the air pump through tubes. This would shut down the flow of air when in-flowing air is reached allowing for air release. These regulators could be be made to suit or switched out. I’m sorry that I am not as well educated with respiratory therapy.
Hi
Can we use homemade cpap machine in mild covid19
Is it useful or not?
If no what is the standards to make it work?
Too bad it requires login to see it.
What sort of dope does this sort of project on Facebook? The only “people” still on Facebook are Russian trolls / disinformation bots and stupid people. Good luck getting useful technical input there!
So, how do you know this if you are not stupid, bot or Russian troll?
Why do you assume they are neither?
Where can i sign up for this hackathon?
https://www.projectopenair.org/
I say, hook a small air pump like those for blood pressure monitors to a homemade oxygen generator like the one described there : Hydrogen peroxide and potatoes in a plastic bottle. -> https://www.crappie.com/crappie/live-bait/349144-homemade-oxygen-generator-cost-8-a/
The flow rate with those little pumps is much to low. What you need is similar to the blowers used in CPAP machines. Those can be 3D printed- I’ve done it. $10 Brushless DC motors for model airplanes can be used to provide the spin, and drivers can be had for about $10-15. You might be able to get away with BLDC motors harvested from old HDDs.
See: https://drmrehorst.blogspot.com/2018/04/the-mother-of-all-print-cooling-fans.html
hey Mrhorst.
nice link of the BLDC motors. I agree this is a very interesting solution but I do think the material PLA is not the right way to go forward. I suggest Nylon PA12 or PP or even perhaps aluminum for more strenght of the part.
Actually, that won’t work very well. You need way more volume and way more oxygen.
Have a look at this: https://rebelem.com/high-flow-nasal-cannula-hfnc-part-1-how-it-works/
To summarize: commercial units deliver 50 – 60liter/min 21-100%O2.
even if you have a strong solution of peroxide (10%), you need a lot of it for just one day.
Best way to generate your oxygen is by pressure swing adsorption, then you just need a slightly bigger pump, some valving and two zeolite columns.
Also could be very dangerous to breathe. There are potential chemical reactions with the stainless steel.
https://chemistry.stackexchange.com/questions/59305/production-of-hexavalent-chromium-during-electrolysis-using-a-stainless-steel-as
Is good to consider heating to clean the exhaled air from viruses?
Definite info on whether the virus survives outside of aerosolised droplets for long is a bit sketchy, also, what it survives while rendered inactive by some degree of heat increase and can then recover from in more suitable environment is unclear. Thorough heating of a given air input is a bit like juggling greased eggs, because insufficient mixing can occur and you haven’t completely “cooked” portions of it. Sure, you can put air through a heat gun and make it come out at 200C in the middle, but what about the stuff around the edges at lower temp, is that entrained air or stuff that snuck through without getting heated so much. Anyway, though you can probably do it, it seems like it’s going to commit a huge amount of energy to making really extra sure you can do it.
If however, we only have to worry about the droplets. Advice so far saying they only get about 2 meters before dropping. Then we can use a high volume system such as that recommended by FEMA in some of their home nuclear bunker construction materials and use a duct with a number of baffles in it. This is to make the air path zig-zag and throw out particulates on the turns. We could fab these up rapidly from steel sheet, and then treat/plate them with a copper sulfate solution, so that collected virii do not fester in there. Additional measures such as hard UV exposure and heat could also be applied.
A uv led might be more effective, won’t heat the air.
Pass it through a UVC sterilizer?
We need a list of charges like for a building. (Maybe an online mindmaptool that can be accessed by group)
Technical
(liter air/minute, pressure in -out, heartrate versus breathrate, Uv and ultrasonic decontamination in and out, ectrolyse with blockwave frequency for O2, measure O2, CO2, NO2, humidity, temperature , exact temperature for warming with IR, generate sterile humidity , essentialoil additives
Medical
to finetune the use in function of the patient
https://youtu.be/okg7uq_HrhQ about ARds
Tools
Airtubes to create a harnass
Aircompressor
Airpumps aquarium
UV lamps
IR lamps
Ultrasound source
Electrolyse with blockwave and efficiency trim
Piboard with i2c to measure several sources…
Tubing that stays sterile
Then the available tools that can be turned in to use for it.
Electrical requirements per device will need to be reviewed for the design of any device. The hospital electrical system is not designed for an overload of circuits.
What we do not want to happen is too much electronics plugged and create a power outage due to overloaded circuits! That would be worst than not having enough ventilators.
Good luck certifying it on each commit.
I think the idea is to have these available just in case people start to worry more about dying than about certification.
Outside of our developed countries where we should more or less have enough equipment and drugs (if we look at italy we don’t but thats another story) but think about 3rd world, if this virus gets to Africa, Bangladesh, refuggees in Syria they are fucked and will take anything over rolling over and dying. Think about poorer people in bad places we as fellow humans have moral responsibility to help them survive.
I’m a novice DIY type volunteering in North Africa. If any of you can provide a super simple set of instructions and a parts list, I’ll personally put together a few of these emergency ventilators for the local nurses. They’re completely unprepared and are frustrated that the docs are already turning away anyone with a mild temperature showing up at the locked front doors. Be glad you’re all in a place where you can still go to a clinic or hospital. If it’s any help for the discussions, I’ve got an old phillips CPAP machine to work with in a pinch. I’m assuming that everyone will already be infected by the time anyone seriously considers using this thing and that transmission will be less of the concern.
http://blog.modernmechanix.com/diy-iron-lung/
this diy wooden iron lung saved lots of lifes in the 50´s polio epidemic in 3rd world countries
Hi all….
Kinda related and kinda a hack!
I work in a hospital in the UK, we make extensive use of numeric keypad/door entry systems, I have designed a key/fob type thing that can be 3D printed and then used to open the keypad doors without touching either the keypad or handle.
Hopefully I can make a few changes to the design and have it up on Thingiverse later tonight
Wow, good job
Actually, I can’t believe hospitals are using keypads for entry.
Not secure (or auditable, etc), and a rather obvious contagion risk.
Nothing is really secure, and properly cleaned keypads (as everything should get in hospitals) are safe enough (though obviously far from ideal).
What keypads are however is really practical – anybody shuffling into that area that needs to know can be told. If you went for ID card with mag stripe you would need an army of ‘technical’ staff to keep verifying, autherising and deauthorising as the medical staffs job roles shift or everyone on staff can just enter any door (which may or may not be acceptable)… Rather inconvenient and no more secure if all you need is the right card or clone of.
We have ID cards for almost 2k staff 4 guys in IT manage it while doing everything else around our network, there are separate groups for hardware and web site. Problem is when you introduce sollution and need over week or two generate cards for thousand or more folks but once its set up and you don’t have big personell rotations then new people and leaving of old is managable.
As Foldi-One says…they are really convenient, they are mostly used in low security areas… i.e. our IT Office (lol), the cleaners and non dangerous item stores and area like that.
Mag swipes and good old fashion keys are also widely used.
I’ve just dropped round to estates and they have given me an old handle/knob so I can test fit at home and don’t need to keep bringing it to test fit :)
Yes, I’m dreaming up some sort of slim boat hook knuckle duster to open all the pull doors as work to avoid contamination. I’m always frustrated that after washing my hands I have to pull a door handle to exit the canteen or toilet and touch all the germs the non hand washers leave behind…done it
https://www.thingiverse.com/thing:4217660
Like this?
https://www.amazon.com/Kooty-Key-Touching-Surfaces-Carabiner/dp/B017QE9D7I
Ahhh, Yeah… That’s been pet hate of mine for ages.. Having to hold/pull the door handle when leaving a public toilet.
I always wondered why they where arranged like that, thinking that it would be better to hold/pull the handle to get in then use your foot to push the door open on the way out (saving having to touch a dirty handle with clean hands).
Then someone explained to me they are done like they that so if someone collapses or needs assistance whilst in the toilet then its possible to kick the door in…. I guess it makes sense : (
Actually, virtually all bathroom doors have an easy to unlock mechanism. Usually it just takes a screwdriver or screwdriver-like object to unlock it. If you were worried about someone that collapsed, you probably wouldn’t want to kick the door into their head. No, bathroom and most other doors open inward so that you don’t slam the door into someone walking down the hall when you open the door.
no it doesn’t every toilet door i saw for past 20years(before in commie times we had usually just metal hook or latch and in 90ties we didn’t had money for remoddeling places so old buildings had old solutions) has lock that can be opened with coin or any other screwdriver like object from outside.
My epidemiology teacher used to say: once you’ve finished your degree in microbiology, you’ll either be the sort of person who opens doors with a handkerchief or the sort of person who eats food off the floor, and if I’m doing my job right, you’ll go buy a handkerchief.
I almost always wear a sweater, mostly because I can open a door with my sleeve. Turn on/off lights, move chairs, whatever. I’ve gone the last four days without touching any object that any other person has touched, outside of my house.
Hi I am some one don’t know anything about MD.Do you think with this problem some of poor country can made VENTILATOR using fish tank Oxygen motor?
Hmmm if it gets down to homebuild being a necessity, wouldn’t the old “wooden iron lung” approach be preferable? http://blog.modernmechanix.com/diy-iron-lung/
Something is messed up with the second page on that site, another copy https://archive.org/stream/PopularMechanics1952/Popular_Mechanics_01_1952#page/n259/mode/2up
The diaphragm is made with the inner tube of a tractor tire. This is awesome.
Maybe there’s ways of updating the design. For instance a diesel iron oil tank has the same or larger dimensions as an iron lung. There’s also quite a few slurry tankers around that have failed from rust or excessive vacuum. these use an iron maintenance door with a rubber pressure seal. remove the door and doorjamb assembly, weld it on to an oil tank.
How about using subwoofers as the diaphrame and pump motor. You will need quite a few drivers, and if you don’t displace at least as much air as the lungs take, you will actually worsen the situation, but on the plus side, control is super easy. At least the Post COVID19 party won’t lack in DIY bass bins.
That sounds like a technique that’s used in some respiratory conditions with a vibrating cuirasse around the chest. Not sure that rapid and shallow respiration would be much help for this. The iron lung approach itself is a bit marginal but combined with a rigged oxygen tent may work for some patients. Real advantage is that for DIY it’s non-invasive. I tend to think that early support with such devices might prevent need of the better stuff later, but I’m not a Doc.
So, not sure really how slow you could drive those subs with their normal armatures. I could see how several might offer enough air movement, but unless they’re moved at a few hz, not how they can make any pressure. Unless you’re thinking of fast valving, so they build pressure over a few seconds while running at their lowest typical frequency.
They can drive as slow as you like, vibrations can be an extra feature, the low end of the response is limited by travel, this is why you would need a lot of drivers. A pure guess is 12 x 12 inch drivers. If the drive voltage is low, the motion is slow, you can basically drive them from a DC source. Switch polarity to change drive direction.
the voice coil needs to be moving fairly fast to keep it cool and not burn up after 10 minutes
My thoughts too robert, I realise not everyone can get everything everywhere, but tryna replace a $100 utility motor with several hundred dollars worth of large bass cones doesn’t seem to be worth much thinking about.
@Murray the idea of using this speaker diagram is extremely clever. To increase the volume of air, all you need to do is increase diaphragm size which you realistically do. The mechanical “engine” of the speaker is the voice coil. I could imagine attaching a large piece of foambaord to/in-place-of the existing subwoffer diaphragm with a “flapper valve & hole cut into it”. You you then place the speaker at low hertz “song” using whatever existing amplifier you have access to.
There is a device with four linear actuators that does like this, expanding a diaphragm over a cuirass. I was not able to find a link for this device…
With all things medical comes a huge degree of liability. Fault detection and alerting are an absolute must.
Careful not to overlook the point of this thread. The goal is not to produce a medical-grade device to complete with things out there, the goal is to provide options to folks who have no other options available to them.
careful with warm water and legionnaire disease
While corrosion of components could become an issue, that could likely safely be controlled by using a saline solution. Most salt should be left behind & what does get ingested would be safe, potentially even beneficial for any virus present in the throat.
The FDA would like to have a word….
If the numbers are correct, most countries will run put of ventilators, and 5% of infected will die because of it, we are talking millions of people dying. So I think here well thought DIY should be acceptable.
Considering the people dying here in the U.S. are mostly in nursing homes, you won’t be extending their lives.
Same in Italy where the Median Agae is 80 of those who died from the virus.
These people already were at death’s door.
Sad to say, but there’s probably a percentage who were on “borrowed time” as it were, who even only a decade or so ago would have already passed at this age due to flu or pneumonia. Now we’re more widely vaccinating for those, they have lived several years longer, but it did not subtract their vulnerability to viral illnesses altogether. So it’s a bit like some “Final Destination” crap, that a virus that does pretty much the same as those killers of the elderly that we defeated (or at least bluntened) turns up.
It’s more than this. Young people *are* getting critically ill. They are having respiratory support. But they survive.
Triaging is happening and some of those who are older or with certain comorbidity are not making it into critical care beds and are dying.
If you (maybe rightly) target your critical care beds to those who are most likely to survive you must not use the mortality of those you neglect to justify this after the fact.
A common pattern in mortality is rising clearly with prevalence critical care is being saturated.
The UK has 5-10 thousand critical care beds depending how you count it ( not including private, coronary care, renal beds). Most in London.
Latest stats are 6% need critical care (14% seriously I’ll), so if only 2% of London’s 8 million residents are infected and 6% need critical care with an average stay of 5-10 days….
Well you can see where I’m going.
jury-rigged ventilator vs. nothing at all?
Yep, nothing at all. Like cancer drugs, they would rather you die a slow painful death than try a promising new but untested drug. I’m glad the government is looking out for me.
If it’s untested it’s not promising.
Testing it means using it. In this situation, no shortage of volunteers. The question is how much risk margin you can expand in accelerating tests while still having enough chance it’ll be at least more positive than negative in outcome.
You seem to be forgetting that we are trying to hit a moving target. There is no reason that the ‘Maker Methodology’ can’t also be applied to the other aspects of design such as Requirements Gathering and staged certification. Talk with medical liability lawyers and hospital admins in order to figure out what type of exemptions, waivers and device self-diagnostics could be put implemented given the circumstance.
The rigidness and inflexibility of the traditional design approaches utilized by manufacturers is as much a function of assuming the underlying requirements are static. They aren’t in the maker space.
There are mechanisms to get unreleased drugs to people who want to give them a try.
Wonder what would have happend if the Generals planning the D-Day Invasion looked at each other and said, “There are no mechanisms to get us onto that beach, past those obstacles.”
James Kirk, “Let them DIE!” – Amazing.
The FDA has a habit of messing good things up royally…
There is a promising paper from 2015 that looks at using Ultraviolet Germicidal Irradiation on N95 masks, with the goal of re-use. Seems promising. My local makerspace has a bio-containment hood with a built in UVGI light, as well as some baby bottle sterilizers, that we are testing on N95’s currently.
The paper in question: ncbi.nlm.nih.gov/pmc/articles/PMC4699414/#S1title
How are you testing?
Touche’!
-Separating the N95 into its various components (strap, valve, mask etc)
-Cut each part into medallions, strips, pieces etc
-Place a piece under UVGI
-Inspect material under a microscope
-Repeat until the material fails.
This recent Chinese paper recommends 70 degrees celsius for 30 minutes, and recommends against UV https://mp.weixin.qq.com/s/3QYVWO4kj5qwuSHnhcM9uQ
As it is sunny today, my thoughts switched to natural UV exposure. However, hanging stuff in your windows is no good because decent glass blocks most UVB. Also if you’re nearer sea level, you’re not getting a lot through the atmosphere anyway. But, total last resort, got no other way to do it… saran wrap (cling film) taped over a cookie tin and leave your mask in there a full day of sunshine might do something. But as pde points out in that chinese link below, no way to guarantee the penetration and depth of sterilization of any UV source. So it’s surface cleaning only. May be acceptable for personal use gloves or something. So why saran wrap? Well according to random interweb results, the classic non-recyclable saran wrap transmits anywhere from 80-95% of UVB… and why cover at all? well if you’re okay with flies leaving poopy footprints or birds crapping on it, you needn’t. Why cover a cookie tin? (biscuit tin etc) … the hope being you turn it into a little solar oven as well as enabling UV exposure, so you’d be low-baking it as well as irradiating it. Use better methods, or fresh gloves/masks if available.
Paint the cookie tin black (inside and out) to improve the baking.
Can do, but the typical shiny metal finish will be bouncing any UV at all angles and might get it behind it and under the first layer of fiber by side illumination.
You could separate out the UV B and/or UV A by using a “blazed grating”, which is a sawtooth profile on metal. The spacing of the sawtooth wave determines the (somewhat broad) UV light wavelengths that are diffracted away (from the conventional reflection angle). Look up “blazed grating” in Google Books for a book which has the formulas.
I recall Wikipedia’s pages as saying that the atmosphere prevents UV C from reaching the ground, but that (some) UV B and UV A does reach the ground.
My thought is to concentrate the UV B and A with mirrors, as is done in a solar-powered oven
It’s not too hard to 3D print blowers that can move enough air quietly. I copied the blower from a CPAP machine and drove it with a motor from an HDD and got a lot of quiet airflow, but the HDD motor is maybe a bit underpowered for this application. BLDC airplane motors that sell for about $10 can be used and driven by $15 drivers.
You have to be careful to monitor and limit the pressure because a little bit too high pressure can burst a lung. That’s why CPAP machines are regulated as medical devices- they are capable of doing serious damage if they are not set up correctly.
Need to find a motor that’s at least intended for continuous duty cycle, model plane, drone, RC car motors really really aren’t.
This is likely going to mean a motor twice the size and weight of what appeals to a hackers sense of efficiency.
The CPAP blower I modeled the printable unit on had a 24W motor. Putting the motor inside the blower where it is continually cooled by the air it’s moving keeps it running cool. I suspect that if you used a 50W or so model airplane motor and ran it well below rated current inside the blower, it would run just about forever without problems.
In what way RC car/plane/drone motors are not suitable for continuous duty?
Their thermal capacity is not so huge, they’ll certainly reach their stable temperature in just a few minutes of use, and they are continuously used longer than that. The bearings will give out with time, but that is a matter of load and bearing quality and would apply to any kind of motor.
“They last for years in a plane” Count the hours, it might not be even a solid week of run time.
A drone motor is several 100w… Then your lungs just explode from the pressure. I think at a lower power they will run a long time.
What about high static pressure server fans? They’re built to run 24/7.
Measuring the pressure of the air might be challenging. Industrial/automotive pressure sensors are, most of them, for much higher pressures and are not sensitive enough for this application. But building a vertical transparent water tube would do the trick (communicating vessels). To measure the water high a simple UV led+receiver would tell the system “this pressure (water height) has been reached”. Add 2 or 3 led+sensors and you can effectively control the pressure with less than 10US$ in material. Aim for 30cm of water. Normal CPAP devices operate between 6 and 15 cmWater pressure.
You use a weighted flapper relieve valve, balloon or similar to limit the absolute max pressure applied to the pipe going to the patient. It seems likely that you won’t have a good seal into the patients airway anyway as you are providing an oxygen enriched stream of helper air into the airway to assist normal breathing in all but the unconscious patient..
My oven uses very low pressure (or vacuum) switches. Amazon has (had?) HVAC pressure switches for cheap. The ones I use range from 0.1″ of water column to as high as 10″.
I think the water depth sensors used in washing machines might work, and there is the old standby, the Pirani gauge. That’s just a an electrically heated wire. Gas pressure causes the wire to be cooled by convection, this causes its resistance to change, and its resistance is a measure of pressure.
Why is HAD even posting things like this? Medical devices should not be part of HAD. A waste of time since nobody should be hacking, modifying, or creating medical devices … “nobody” meaning most of us that view this website, myself included.
Sure, medical devices are best left to the experts, but when they can’t be found or afforded and all else fails why not? I work on a sheep farm and I’ve had problems during lambing season. After consulting the veterinarian they recommended euthanasia for complaints that other farmers solve routinely. I don’t know what’s wrong but it appears to be systemic.
I think we found the FDA employee in this thread.
No, just a guy who is using his brain. First off most of you have zero medical experience and zero experience with medical instrumentation. You don’t even have a clue when to use such equipment or when not to.
Let alone getting it certified.
You think a hospital or clinic is going to allow you to roll in your home brew ventilator? Hell no. They will call the cops on you and probably sue you for good measure.
But will they allow you to put your own ventilator on grandpa after the hospital has said “we have no more space, all ventilators are reserved for people with best chances of recovery”? That is already happening in Italy.
Uh……gaining knowledge and “getting clues” is a fundamental part of Hacking. Duh. The pedantic dismissiveness in this specific thread is extraordinarily ignorant and selfish. When/if the open source community develops something that can be used (albeit temporarily) as a rudiementary stop-qap solution to help ease suffering and perhaps deaths, when your kids is laying there gasping in front of you (becasues no “official/perigreed/certified” devices are available), be sure to very clearly demand the hackers to “get that thing away from my child!”. Jesus.
Lol because all the people on hackaday are doing nothing but browsing the web a day. A lot of readers ARE the people building such devices and we might not be talking about western hospitals here.
Uh huh, no one has ever hacked an insulin pump. Also there are no medical devices with severe design deficiencies. I am with you on this one, myself included.
I’m just saying that medical devices are not a good topic for HAD (Hack-A-Day). Anyone can go do whatever they want in the privacy of their homes, but HAD shouldn’t be opening this up, especially to inexperienced tinkerers.
+1 if the FU was directed at me … I hit someone’s nerve.
Found someone that never went through the “do it yourself or or be left suffering” thing. Let’s hope that whatever happens in the upcoming months doesn’t change that for you.
As a medical professional who specializes in implementing, maintaining and sustaining patients on mechanical ventilation, I would have to agree with Max S.’s comments 1000% after reading many of the responses to this HAD “project.”
Totally agree (retired product designer) this is not a hack, be smart – copy whats already been designed and tested as fast as you can. Give the plans out to every manufacturer and supplier – if you want to help get to the factory. Let the legal guys work out who owes who money afterwards
Founder / CEO, FLEDGE Innovation Labs
Medical Devices Incubator
40+ years developing / commercialising medical devices
=====
Max S and Steve R are 100% correct …
This is not a DIY project.
We cannot solve this problem using garden hoses and vacuum-cleaners, or by passing exhaled air though buckets of boiling water.
See my post 21 March.
I am getting all the messages posted, but if your in a position to do engineering drop me a line,bill2resist@gmail.com
Hi. I dont think that you’re getting the point. The goal is not to build a replacement or competitor of commercial available ventilators. The goal here is building a survival device, in a broad way, that can be mass-produced in a low cost and be easily reparable, for war times like this one. This device can kill people? yes. But more people will die if this device is not created (check the post of the people in hospital that is hacking the regular ventilator to make room for 4 people).
Also, it does not need to be something fancy. Maybe something like a iron lung used in the 50’s, with a very low tech and easily to be repaired, can save thousands of lifes.
Thanks for commenting Dave.
With respect, I ABSOLUTELY do get the point …
In Italy RIGHT NOW – TODAY – there are 400+ people being admitted to ED with dyspnoea, and oxygen saturations below 90%. This rate is doubling every 3-4 days.
There will *never* be enough ventilators to help everyone.
There will *never* be enough iron lungs to help even a fraction of these people.
There will *never* be enough time to build a ventilator solution and deploy it, or enough people to implement or manage it.
Tragically, only 3-4% of people who are ventilated will survive.
A hundred people have died in the time it took me to write this reply, because their O2 saturation crashed.
Ventilation is an invasive, resource-intensive solution. Its not just the ventilator – you need a skilled person to manage the device and the patient. Its a lot more than blowing air up someone’s nose.
This hack has digressed to a technology-driven discussion that address the wrong question …
Take a look at the original brief – which describes a NON-INVASIVE high-flow nasal cannula, not a ventilator.
>>> WE DO NOT NEED TO BUILD VENTILATORS <<<
We need a way to provide respiration support to KEEP PEOPLE OFF VENTILATORS.
We need something simple and inexpensive – $50 – where production can be ramped up by *orders of magnitude in a matter of days/weeks*.
Trying to cobble together a ventilator from bicycles tyres and duct tape is not the solution – it will *never* be supportable or scale to meet the need.
AND – it will leak virus-loaded aerosols that infect other patients and healthcare workers – meaning the balance will shift from people being carers to people being patients – which will implode the healthcare system, accelerating fatalities.
Forget trying to build a ventilator – that is just not what we need.
We need to develop ways to provide oxygenation support to PREVENT people from needing ventilators.
I Agree gary Jones, its why i´m going to make this Wood Iron Lung and keep it ready for use here in Brazil : https://archive.org/stream/PopularMechanics1952/Popular_Mechanics_01_1952#page/n259/mode/2up
Because in Australia its estimated we will be down about 2000 ventilators. The thread isn’t “commercial vs home made” the thread is ” home made vs no intervention”
A bit nuts really all this on the motors / drivers overheating motors from drones – homemade fans just get a decent compressor from machine mart control the air flow and hey presto you have enough air for hundreds of people ?
Get a large grocery bag, that holds about the 4 cubic feet a “decent compressor” that doesn’t need industrial wiring puts out a minute. Now breathe from it only once a minute, enough?
https://panvent.blogspot.com/
For all the naysayers no one is going to give a single fuck about regulatory shit when hospitals are overwhelmed or in a third world country. This isn’t just for us in our cities with modern infrastructures and readily available essential services.
Well, you don’t want to do more bad than good. If you use a crummy device, then you could end up causing more deaths than if you used nothing. Without proper testing, it’s hard to know if it’s more bad than good. You don’t want to just use it and then find out it’s more bad after it’s killed a bunch of people.
^ this
please, please, please- use ur ingenuity to increase the uptake of hygenic processes of the mass population. The medical community’s goal is to slow the rate of infections such that the ventilator supply is not maxed out and therefore triage doesn’t have to decide who gets limited resources. Medicine isn’t about glory or click-bait’y; but it is about decreasing morbidity and mortality. I repeat, figure out how to slow the rate. You’ll be a much bigger hero from the ppl who never knew you saved their lives. And you don’t need an MD to do this.
+1
Good point!
There must be loads of simple things that we can create, invent or implement to make the spread of the virus slow down.
This, everyone seal themselves in, LOL https://youtu.be/gbL6rwGJpIw
This
Thank you Doctor Clint – There are hundreds of HAD posts here and after a week of posts, still not ONE drawing, specification, process sheet to build anything, let alone a ventilator. It is a testament to how badly our educational system has failed us. Does anyone here have an engineering degree, medical degree, any high volume manufacturing experience??? Anything??? Anyone??? ..,
Hi, I am looking for a team to put together without wasting time, I have a design and been evaluated by Medical professionals. I need engineers and at least 1 MD, prefer military background or trauma. Anesthesia. Lots of garbage on the site, but I am moving forward, email me if interested. Bill2resist@gmail.com
Try this website they are sometimes resourcefull. They supply military customers in comecial diving applications. They do not have exact equipment, maybe a long shot, but can possibly design or reengineer someting existing. My husband used to work for them. They might be closed due to lockdown so try to find some personal contacts in the site. Their parent company is Divex in Ireland and they are based in Cape Town.
DIVEX OCEANICS (PTY) LTD
Montague Drive, 11 Dawn Rd, Milnerton, Ind, 7441
021 551 2233
https://g.co/kgs/RGk1kX
I have a mechanical engineering degree, access to rapid prototyping equipment and experience leading small development teams… of course, never before in pursuit of such an impactful and time sensitive goal. I also have a few fellow engineers who are interested in doing more.
I agree with your frustration, but I wouldn’t blame anyones education. In general, I would say that it is difficult to organize, plan, and hella hard to execute and complete a development project.
Problem solvers need boundaries to open up our creativity, and specific problems to solve.
I’ve seen a couple of posts asking essentially for the specifics of how a ventilator works and what are the target requirements for a hackaday version. I’d love to see this article/post updated with those essentials.
One comment to the naysayers. A medical grade piece of equipment must last for years and probably has countless features to make it a more useful and valuable product. Whatever is hacked together won’t compare. Instead an inexpensive ventilator that can safely supply the proper mixture/pressure of oxygen for just two months could make all the difference in our world.
Gosh.
all those fancy names for a glorified air pump.
If you’re thinking of hospitals full of these, I’m, thinking of a regular industrial compressor and a bunch of PVC pipes. It would need some extra plumbing and safety stuff of course, but that’s much easier on a large scale.
So if you’re serious about this, then skip the usual suspects and put some doctors who know what they need together with engineers which have experience in industrial equipment.
You can not use a regular piston based air compressor because of issues with airsole oil droplets. You could use a [cleaned] diagram based hardware-store compressor, but these are less common. I am onboard with your PVC plumbing ideas, that part is fine :)
What if you ran it through a filter to trap the oil?
See scuba compressors, I breath it all the time…
Has anyone considered using a midi clock (music equipment or music software) to regulate how often the air is dispensed?
If you need any sort of timer I can code up something to run on a PIC in a couple of hours.
I am interested in helping out! I could deisigna all the electronics needed for such project. If you are interested , give me a mail on bflorin520@gmail.com and we could talk more.
And just think of how all this research will help all the far more deadly virus’s like the flu.
The reason influenza is more deadly than this is that more people get the flu. At the current rate of spread of covid-19, that will no longer be the case in about 30-45 days from now, at which point more people will have or have had covid-19 than the flu, and covid-19 has about 10-40x the mortality. It’s not likely to be as bad as 1918 as regards proportion of the world’s population killed, but I wouldn’t be surprised if it ends up killing more people overall, simply because there are so many people.
I’ve seen quite a few estimates and have run my own, and it’s really heavily dependent on what dataset you use, but most of us are coming up with numbers indicating that the date at which 50% of the world will have it is somewhere between April 20 and May 15.
May 8th (+- 6 days) until all beds are at Max Capcity.
Try paying less attention to Trump and more to Fauci.
Absolutely!
To design we need technical details:
1. Max flow rate 6lpm
2. Max allowed pressure???
3. Desired humidity level???
4. Oxygen mix range???
I’m looking but don’t see these numbers uet.
This is what I’m wondering about as well.
I’ve got a working prototype made from a high-volume manual pump typically used for inflatable mattresses and inflatable rafts, driven by a simple “piston”(a spinning wheel with a rotatable elbow, like a steam engine) that is powered by a geared DC-motor from a drill which is being water-cooled.
By NO means is it a perfect device, but in an emergency I would prefer it over having nothing.
Currently, I’m working on adding a way to humidify the air and a way to set a pressure range/breathing speed.
for nasal cannula
1. 20-60Liters per Minute
4. 21-100% FiO2. 21% is the oxygen concentration of ambient air
for CPAP / BIPAP
2. I suggest 40mmHg as the max pressure. 30mmHg is the actual cut-off for safe ventilation but sometimes we need to ventilate with higher pressures
4. 21% to 100%, see above
Those variables are machine and patient specific based on anatomy, physiology, and pathology. That is why the machines take years to correctly learn how to use, safely.
For all of the people commenting about medical certification. The stuff such as ISO13485 and 21CFR820 (QMS), 93/42/EEC (MDD), 90/385/EE (IVD), ISO14971 (risk management), IEC60601-1 (general safety), IEC60601-1-2 (EMC); not to mention the myriad and multitude of other standards and regulations scoped for the specific type and class of equipment.
I have been on projects (including ventilators), where product certification and initial audits comprised over half of the development costs. Then there are the liability insurance, recurring audits, and continual regulation and standards updates costs.
These costs are borne by the same consumers that demand *BOTH* rapid response from the FDA and medical equipment designers and a high level of goddess-like fail-safe performance.
Thank you. 62304 for software, too.
Get started then, crash program 8 days a week 25 hours a day, accelerated compliance with all that mess and in only 6 months you’ll be ready to go, meanwhile…
https://www.youtube.com/watch?v=shs7VQhVvxA
And my personal favorite, ISO-60601-1-4. I have also worked on medical devices. I don’t want to poo-poo everyone’s enthusiasm and desire to help a cause, but until you’ve been in it, you really don’t know what it takes to design, test, manufacturer, market and distribute a medical device. The “labeling” requirements alone give me an ulcer. There MAY be some space for open-source design (there’s nothing wrong with a design being open, as long as it’s gone through the same standards and you can 100% verify its provencance), but I just can’t see anyone manufacturing a legit device in their garage or maker space. This ISO-9000 is hard? Try 13485!
Thank you this needed to be stated.
Sorry, pressed the “report” button in error.
Stuart I am a mechanical engineer en also designs systems for hospitals.
While complying with the applicable ISO’s is a must for equipment in official use, this is one case where the need can become so very big that there will simply be no time to go through all those loops and that any good design, will do.
I can assure you, if you have no other way and you need to choose between nothing and a device that can work but does not comply with ISO, you will probably take your chances too.
I know I would.
But it’s not up to you. This would set a terrible precedent. It cannot be allowed under any circumstance. I’m not for throwing away lives but medical devices have to be 100% foolproof. And for that, it probably takes a decade of testing. Why you ask? One word. Trust. Suppose you design a machine and make a lot of them. It works, at first, but then fails in the same way for everyone. It kills all of those people down to the last one. You think it was the virus but find out later it was the machines. Word spreads. Now, trust is broken. People don’t trust hospitals anymore and avoid them. Conspiracies fly. They refuse to vaccinate. Trust is gone. Many more people will die simply due to lack of trust in hospitals and doctors. That’s why standards are set so high. They have to be. Without trust, modern medicine fails. The best thing to do is educate people. I saw at least 20,000 at bars today. People everywhere. All those people could have been at home if someone provided them the right message about why. Nobody did. There is no one taking charge. The emergency broadcast system should have taken over. All stations should have broadcast the same thing on every station. If there had been a nuclear explosion, we would have done it. During 9/11 we shut everything down. That was arguably a tiny disaster by comparison.
Quite right.
What about managing precedent as it arises, or some sort of unorthodox sociological/psychological thinking for dealing with that itself as some kind of “disease” to be modified/therapied in some fashion?
“….but medical devices have to be 100% foolproof.” With respect, this is simple ignorance. NO DEVICE is ‘100% foolproof’. It’s about simple reliability metrics and margins of confidence. This isn’t magic nor does it require 10 years of medical school. Medical device reliability is a function of Highly Accelerated Life Testing. If you provided an open performance specification which detailed the tolerances and testing thresholds a machine needs to satisfy, you’d be surprised as the designs engineers and Makers would produce in record time.
I’m not qualified to tell you what is medically feasible and YOU are not qualified to dictate what is technically feasible. It is far easier to say, “it’s impossible” rather than acknowledge where your expertise ends and the expertise of others begins. Instead of providing such USEFUL information and documenting requirements for such a device, you are so convinced of your own arrogance as to think it takes a PHD to design a product which conforms to a set of clear requirements. It does not. It only takes clear requirements and competent engineers/technicians.
Actually, it’s not just about reliability metrics …
It’s about developing products in a QUALITY-MANAGED development environment.
You can’t build something using a home-made design and parts from Walmart and then expect to get it certified …
The DESIGN PROCESS is at least as important as the quality of the end product.
Whether a life-saving piece of equipment needs to be certified in these circumstances is another question.
The problem here is to KNOW WHAT YOU DONT KNOW – which is a challenge for well-meaning people who have never done anything like this before.
If we need more ventilators, then we need to support people who ALREADY KNOW HOW TO MAKE VENTILATORS.
https://newsroom.resmed.com/news-releases/news-details/2020/ResMed-Statement-on-COVID-19/default.aspx
We need to support their supply-chains and distribution networks which are in danger of collapse.
We need to support people who can build them, test them, get them to where they’re needed, train people and support them. AND – make sure there is enough PPE and STERILE lines etc to operate them – esp if patients are being intubated – so we dont MAKE THINGS WORSE by introducing bacterial infections to already compromised patients, or by producing virus-laden aerosols that will infect health-care workers – turning them into patients and causing collapse of the emergency healthcare system – which will INCREASE FATALITIES.
As appealing as the idea might be, this is NOT the same as modifying CO2 scrubbers in Apollo 13 – which faced a single problem that required ONE solution, backed by thousands of experts solving ONE problem – with a single point of delivery and without the risk of killing the people trying to help.
This is because in *normal* circumstances, we ideally want everything to be *as safe as possible*. If we don’t have to make something unnecessarily risky, then we shouldn’t. But these are not normal circumstances by far at all (and exacerbated in such by the utter ineptness, slowness and brokenness of our government). Here, the relevant design criterion is “an expected value better than nothing (and not worse)”.
Fine. But a few months from now, when 5% of the 1.4bn population of India needs a ventilator, no-one is going to give a damn about certification. All that will matter is efficacy.
I was thinking we go “OLD SCHOOL” PEEP/Super Peep with a trash can filled with water. Length of tube and depth in the water regulate the pressure.
NRPR elbow, with anesthesia bag and one way valve and adjustable pressure valve.
Granted, not technically a ventilator but if CPAP/PEEP is all that is required many ways in the old medical texts to DIY pt. care.
If patients wearing masks actually does anything to prevent aero transmission, then I don’t know why CPAP is ruled out, since the masks on those could be covered by a normal face mask.
But I agree, digging back a little into the past will find us the simpler devices that are easier to jury rig.
There are currently concerns for NIV (e.g. BPAP) / HHHF (e.g. AirVo/Optiflow) use in COVID-19 having worse outcomes.
Open source *invasive* ventilators may be of use, assuming any hospital dares to use them, once we run out. I have no clue how we verify and validate the software and hardware, though, to the safety standards we expect…
It’s not about the technology – it’s about the regulations and threat of being sued into oblivion.
You accidentally ended your sentence before it was finished. I’ll finish it for you: “it’s about the regulations and threat of being sued into oblivion because you killed all those people with your pile of untested trash.”
They are currently testing drugs on patients who are dying with covid-19. Testing. Being a doctor is about access to knowledge. You think the average nurse, doctor, health worker knows ANYTHING about anything being talked about here. Theyre guessing too. Panicked guessing. People are dying, yall need to stop just being neg and devote your time to any kinds of solutions or your fam/friends will die too.
Paramedic
Flight Paramedic
Paramedic and A&P instructor
ACLS instructor
EMS system chief
Fire & Rescue Capitan(now in med. ret.)
As a backup to an automated vent there is always a bag valve mask(BVM) available in the ICU/OR/ambulance to manually ventilate an anaesthetized or intubated patient.
After thinking of designs along the lines of a modern vent I decided for this situation an old school iron lung would be most reliable. There is a reason that they went with that design in the old days and kept it for so long, it is very reliable and safe considering how simple and cheap it is, it is also easy to manually pump in a power failure, way easier than a BVM and there is not risk of extubation and maybe tubing the esophagous(patient dies in ~4-5min) when a human ventilator gets tired and maybe yanks on the tube. The only big downside is mobility, but we are not talking about a life sentence in the ‘lung’ in this case.
It is really important though for a high patient to care ratio operation that alarming be based on capnometry(exhaled co2) as o2 sat can stay near 100% for so long in an insufficiently vented patient while their blood co2 acidity pickles and kills everything except a slowly dying brainstem.
As for oxygen, yes any airgas operation can produce plenty for any medical need but probably not certified, so a cheap way to verify purity and safety would make things better.
So if there is a mass need for ventilation I suggest
-DIY design for iron lungs for ventilation(a simple Sten gun engineering; from standard parts design)
-industrial oxygen supply
-shotgun airway tech courses(1-2 days) for EMT basics and other first responders or medical workers to manage a large number of people on vent
Important to rotate the emergency airway techs every hour or two and have a good strict oversight so they can’t easily space out.
How about a cylinder large enough to hold a human with a simple rubber oneway valve inside (think sucking chest wound-style) and a large rubber diaphragm sealing one end. Then…..a bicycle on a stand with an ovalized drivewheel which would alternately push-then-pull on that diaphragm? Could easily (though admittedly: roughly) be calibrated to something at least reasonable. We does what we has to.
So about the iron lung: was invented originally to treat patients with polio-induced paralysis of phrenic nerves (these control the diaphragm). These patients breathed ambient air, and their pulmonary function was intact (compliance, oxygen diffusion etc)
I don’t think an iron-lung type device would benefit a patient in a COVID-19 setting. COVID-19 patients have severely compromised pulmonary function due to massive infection (COVID-19 virus + bacterial superinfection) with concomitant edema. Both of which cause reduced O2 diffusion and pulmonary compliance. I imagine most die in ARDS and multi organ failure.
We therefore need high oxygen concentrations (up to 100%) and high ventilation pressures (up to 30mmHg, maybe higher for a short time only) to the keep all lung segments open and press oxygen through the pulmonary edema to the red blood cell.
In the COVID-19 setting the proper cascade of respiratory treatment, in my opinion, is as follows:
conventional o2 nasal cannula (up to 6 liters air per Minute)>
mask and reservior (up to 15 liter air per Minute)>
high flow nasal cannula (20-60 liter O2 per Minute, adjustable FiO2)>
intermittent CPAP mask>
respirator on CPAP setting (PEEP 5mmHg, adjustable FiO2)>
respirator on BIPAP setting (max pressure 30mmHg, PEEP 5mmHg, adjustable FiO2)>
ECMO
please advise if I missed important points or if you would change the escalation cascade.
Concerning the project I suggest dividing it up into several groups (high flow nasal cannula group, CPAP group, BIPAP group, etc) according to the cascade. There may be several projects within each goup depending on the approach taken (repurposing existing products vs constructing / hacking a new machine), as well as the use case (out-of-hospital vs. in-hospital).
A big concern in my opinion is sourcing oxygen and power in an out-of-hospital setting.
tc
The key spec for an open source vent is that it must be made of parts that are available everywhere already. We might need 500,000 of them in a month. The parts should be things that you can buy at Home Depot or Wal-Mart. The design needs to be developed with medical experts along with a training program, so that a mechanical design, cell phone app, 3D models of printable fittings and training video can be prepared. Also, FDA Regulations and legal liability will need to be waived, so government support Is needed. I contacted my congressman’s office; they send me to an FDA website on emergency approvals. It could be made by a company that manufactures custom pneumatic or hydraulic systems. Or perhaps a mechanic or HVAC tech could make it with online instructions.
We met with 6 senior engineers, CTOs, clinicians & managers each who have worked in the medical respiratory business for 10-30 years. We came up with a couple of ideas. the first one is a modified CPAP machine that may help people at home. It uses an oxygen fortified CPAP machine with a pipe in a bucket or trash can filled with water for exhalation resistance (positive expiratory ending pressure aka PEEP) The capture of the exhaled breath under water prevents the virus from escaping into the room. The oxygen and extra pressure in the lungs helps force more oxygen into the bloodstream for someone who has compromised lungs to hopefully give them more time to build antibodies. This needs a source for masks (maybe thermoformed or 3d printed, or adapted from painting respirators.
The second one is a time cycle pressure limit mechanical ventilator. It could use a shop vac with a dimmer switch for adjustable pressured air supply, modified sprinkler valves for inhalation and exhalation valves, all controlled by a cell phone via the headset connector or some other adjustable timer. A stereo can be used to amplify the signals from the cell phone. (these parts have been tested) This would be used in a MASH tent in the hospital parking lot in case they run out of ventilators. This would provide a peak pressure of 50-100 cm H2O for inhalation and 20-50 cm exhalation pressure (PEEP) The oxygen level would be 40-60%. The oxygen could be titrated with a pulse oximeter, if no oxygen meter is available.
In either case, the patient may need an oxygen supply, which might be suppled via a pipe from the tank at the hospital, or from a tank or Dewar from the welding supply store. If there is an issue with oxygen distribution, fiberglass insulated steel drums could use used for Liquid Oxygen distribution.
These ventilation methods may atomize the virus in the patient, leading to the need to 100% capture of the exhalation into a filter, or perhaps a fume hood over the patient, exhausting outdoors or bubbling through bleach.
Would passing the exhaled air through a domestic microwave oven sterilise it?
Could work but bulky, etc. Ultraviolet Light Kills Virus, bacteria like UV Sun Light. Plus exposed to UV A light creates Vitamin D3 in skin. Which means Pure A Tanning Beds might be good option for Treatment before you even need a Ventilator.
T-Cells scavenge for Vitamin D to Activate for killing Virus Cells! UV Light makes for Excellent Sanitizer! ….UV B/C light damages DNA to kill it. While UVA does but much safer for human exposure. Being in Sun light (as long as don’t burn) makes for great way to be and feel healthier!
It is used in ponds, swimming/jacuzzi water treatment! Hand Sanitizers Works too! Need More Research for a better understanding of Sunshine’s Benefits as well as dangers!
Thanks for sharing this info.
also, possibly related looks like some folks are taking on broad effort via: https://app.jogl.io/project/121#about
Hi, can you tell me, if it’s possible, what kind of O2 sensor can I buy and hopefully be compatible with arduino platforms?
“So if there is a mass need for ventilation I suggest
-DIY design for iron lungs for ventilation”
Plus, when constructed on its own roll around cart it has the advantage of not taking up a bed. Also narrower than a standard bed.
Yes iron lungs worked. What’s wrong with them now. It will be easiest to make at short notice and not too difficult for anybody with engineering and electrical knowledge.
Looking at responses, has anyone thought of a simple modification of adding 2 check valves to a fire bellows device and attaching a flywheel with adjuster to connecting rod that would allow to adjust for stroke length and therefore control of volume on each pump of the bellows. The inlet valve could also have the ability to be plumbed to an oxygen feed system to increase the o2 level. The last part would be coming up with a way to deal with the expelled gas from the lungs and decontaminate… just a thought.
Coould CPAP/BiPAP machines be hacked with software to work as a respoirator? Some BiPAP models are almost identical to devices sold as ventilators. It wouldn’t help the oxygenation, but I think the O2 problem is more easily solved (weld gas, O2 generators being much more common home medical devices)
Leverage COTS… Commodity Off The Shelf… anything that can be re-purposed… are baby bottle liners “sterile enough” to line parts that would otherwise have to be made from sterilisable material or specific non-toxic materials? Could we line a bellows pump with them? Are true HEPA vacuum cleaners suitable for post patient air processing?
Don’t forget that no clinic or hospital will touch your homebrew toy for obvious reasons.
We’re not going to be in your idealised little Kansas any more.
Yeah, these “must be certified” responses are so myopic as to be absurd. Pay no attention to the little men behind the curtain.
I think in Sudan or India, when people die by millions, will be happy to use it even when works just 70% of the time compared to nothing, that means just plain dead.
It would be nice to share the possible 3d printable possible parts projects, so everyone can join in ..
Yeah, a large proportion of non-critical components that can be made easily from any filament on most printers would be a good design goal, to enable “distributed manufacturing” so parts can be made by volunteers or small 3D shops and assembled at point of need.
I have seen so many of these projects attempted over the years, and 3d printing is not what you need. Non-critical components can be made faster, cheaper, and far more durably from vacuum forming, metal or plastic fabrication, traditional machining, or even carpentry. If they are not simply modded COTS (off-the-shelf) parts.
3d filament printing is simply not optimal for this kind of work. I not long ago was working on a way to replace broken hospital bed wheels in Nepal, and suggested using simple razor kick scooter wheels. Cheap, easy, available, and bolt right on. Took a week of fighting the people that wanted to -PRINT- hospital bed wheels using diy filament printers, failed, then tried to print them over wood, wire, and every other reinforcement to keep them from cracking.
All because they had only one god to worship at the altar of, and PRUSA was his name. People died for that vanity.
Hey Manuel,
I made an open excel list with potential 3D printed parts that are needed against corona. If you have something please add towards the list.
https://docs.google.com/spreadsheets/d/1bNjj23e5jFHIf-2XRq_RhuYsdASIoW4t5FKtAd2EiVM/edit#gid=0
Regards,
Willem
You have to get hospitals to install UV bulbs in the HVAC systems first so you can actually make sure it doesn’t spread to other units/floors. Stairways and elevators should have them in use as well..
Second, Ozone, the O3 is very aggressive toward Organic matter should also be used.
N95 masks _CAN_ be reused assuming you aren’t sharing masks (and it’s not soaked in spit, sputum or 100% humidity. )
If placed in an autoclave in UV. Double points if there is Ozone circulating in there.
You should NOT use steam as it will mess up the filter. Part of the N95 effectiveness is that the filter has a static charge and functions great if dry.
A UV bulb/Sterilizing/Autoclave is dumb simple to make, it’s a normal florescent bulb minus the phosphor coating inside.
A Ozone generator is dumb simple as well. A fly-back transformer from a neon beer sign with the terminals attached to 2 aluminum/steel screens or chicken wire on each side of a plexi/lexan will generate so much ozone in 2 minutes the air in the room will smell like a lighting storm and you can get a coughing fit from it. (I don’t need to say large an amount of Amps it generates and how dangerous it can be) a Jacob’s ladder setup also generates Ozone as well obviously.
Aka highly recommend open a window afterward.
The only problem is that the UV and the O3 will “burn” the n95 rubber band. Be advised.
Ah yes, the uncontrollable coughing fits will undoubtedly help those suffering from uncontrollable coughing fits :-D May be helpful for vacated spaces known to have been exposed, and well contained for sterilisation purposes.
sterilization lamps are made of quartz which passes UV-C, while lighting fluorescent lamps are made of normal glass, so lack of phosphor isn’t the only difference. but high pressure mercury vapor lamps (used as streetlights) can be converted to produce UV-C by breaking the outer bulb (the inner one, which has discharge inside, is quartz)
Can a rinse in 90% alcohol assist in cleaning the N95’s?
This is a fantastic idea. One commenter identified that the device described isn’t precisely a ventilator – is this accurate? If so, please update the post so we have a better baseline understanding.
It is really important that anyone with the technical know-how gets involved with this. It’s still unclear how bad this outbreak will get, and working on this now is staying ahead of it.
(as an aside, I am reminded of the scene in Apollo 13 where the engineers make a CO2 filter from spare parts.)
Gotta laugh at the “but medical device regulations!” posts. The idea is not to replace medical devices with these. the idea is to use them for a few weeks then trash them once either the COVID-19 epidemic has reached the other side of the bell curve and regular hospital operations (with their existing stock of regulated devices) can cope, or society has collapsed and device certification is a relatively low priority. When the alternatives are ‘unregulated device’ or probable death, I suspect few would choose death.
In terms of practical short-term usage, the main concern would be contamination of airflow from the passage through the warm water bath. The water would need to be acceptably sterile: straight municipal tap water for first-world countries is likely acceptable, using total-loss circulation (water flows in from tap, passes through the heater to warm it, passes through the chamber where the airflow bubbles through, is dumped out). In the event a constant clean water supply is unavailable, things become trickier. And chemical sterilisation methods for recirculating water would need to not offgas into the airflow (or any offgassing must be at worst unpleasant but not actually harmful). Either passage through a boiling stage or an extremely high intensity UV treatment with sufficient dwell time could work. Design of the bubbling chamber would be tricky, it would need to be sized to avoid aspirating water into the air stream but not so large that a stagnant film could build up in the warm humid environment.
^this….duh.
Yes, design them to last 6 months and hope we’re burning them in 3.
Bear in mind chemical water treatments of teaspoon of bleach a gallon, or 6 drops of iodine a gallon also require an hour dwell time to be effective.
concerning the non-sterile water:
Use sterile 0.9 % saline solution instead (if it’s not corroding your machine). This should still be available in a hospital. I’ve used this as a medium for inhaling horses while testing drugs in my doctoral thesis (I’m a veterinarian). At least it is sterile and because the electrolyte concentration is the same as in the body it is less irritating than (more or less) pure water.
And to all McGyvers out there:
One thing you should all be aware of: We are talking about highly critical human patients whose lungs are already under outmost stress. Every little mistake like
– a certain number of pathogens / particles in the air (filtering ?)
– the pressure being minimal too high for a certain amount of time (can you regulate exactly?)
– other volatile substances in the air (from rubber or plastic) inducing additional inflammation in the lower airways
– accumulating CO2 (dissolves to HCO3- and H+ which changes pH in lungs and in the blood!)
can be the difference between life and death.
Are you aware that maybe you make things worse than without your device?
Just a comment. I’m not talking about regulations but I have ventilated > 2000 horses undergoing general anaesthesia and horses are even more critical than humans considering their pulmonary function. Don’t underestimate the dangers!
Just my personal input.
Essential input! And can some veterinary tools be converted?
Ummm, there’s already a medical grade normal saline (0.9%) shortage nation wide… but good information nonetheless.
Hmmm, fresh black coffee? It’s been heated above 50c, it’s got some natural anti-virals in it, phenols, caffeic acid I think. But yeah if you’ve got spare coffee making capacity you can just use it to hotten the water and throw salt in it.
This. All of this. If you aren’t a medical professional, your time and energy would be better served preventing contamination in your local population. Be the hero today for the person you save from needing a ventilator in the first place.
Hi Dr LeClair, I am a medical professional and working on some engineering projects, looking for a medical adviser right now, Interested ?
how much volume and pressure need per breath at 5 sec interval? is 15L O2 per minute enough for patient.
https://www.instructables.com/id/The-Pandemic-Ventilator/
Already done!
Hydrogen as a medical gas to treat respiratory illness is fairly new. It was used in Hubei China to help treat ARDS. Perhaps it would be good to integrate its use along with regular oxygen with the ventilator and add its settings. Hydrogen gas has been shown to suppress Cytokines. Here is the literature on hydrogen as a medical gas – https://www.frontiersin.org/articles/10.3389/fonc.2019.00696/full
I’m an electrical and deeply embedded engineer with a focus on safety critical systems. My PhD thesis is about software architectures for such systems. I’m willing to support a project if I believe it is feasible. Let me know if I can help.
Hi Thomas-if still interested let me know- have some ideas I am a Respiratory Therapist among other things
Bill
So who is going to pay for the FDA (or whatever is local to them) qualification? The factories that want to sell it will have to get it certified. That is pretty expensive.
You don’t need FDA if you want to produce something that won’t be used in USA. For example, pleople in India will be more than willing to have that option, even if it not FDA-sanctioned (but obviouslty work reliable). Let’s see if someone in USA will let people die because they don’t want to use a non-FDA approved device. By the way, it is kinda funny just see all of those USA-centered minds, when this shit is going for all the world. We are just one humanity, so we need to think like one.
What about producing oxygen by pure water electrolysis (i. e. on graphite electrodes powered by standard power supply) and adding it to patient’s air? Of course there’s also hydrogen produced – it can be used to get part of energy back or, in the more simple device, just released outside the building.
A medical professional can answer this better then I can but my girlfriend friend (who is studying to be a doctor)explained this to me. When given pure oxygen the body becomes lazy. You easily get enough oxygen so you don’t have to inhale as much as you would otherwise do. Because you inhale less you exhale less. This creates a build up of co2 which is bad for your health.
I can say your almost right, oxygen is toxic to especially neo-nates, what you are talking about is in patients with COPD, a disease, too much oxygen knocks out their respiratory drive, however-most patients dont have COPD and if they need that much oxygen-they certainly should not have it restricted, we give 100% to COPD patients understanding the potential
Thank you. As an RT it’s good to see someone else on with the voice of reason. And since there can’t seem to be a consensus of which way to go. I have been looking for ways to put my 3D printer to work. Here are but two sites that have downloadable STL files.
The most promising requires an antibacterial filament to print the mask. Bonus is that it is permanent. Below are the masks that I found interesting:
https://grabcad.com/library/coronavirus-flu-reusable-mask-1
https://www.3dnatives.com/en/mask-against-covid-19-180320205/
https://www.overstock.com/
PUREMENT® Anti Bacterial Orange Filament 1.75mm, a PLA That Kills Germs (Single Pack)
Item #26673934
not sure that you can do the mask with printer, the M95 mask are specific to allow air in but exclude the virus, which is much smaller then the weave of most fabrics,
now one area I would like to see is the body protection system used in the movie Andromeda Strain, lots of reasons-main one is that its patient use-for as long as the patient in the room, its easy to get in and out, saves time and much safer, and can be cleaned and reused. Going in or out of an isolation room is expensive and time consuming, as well as very hard on staff that are busy, also there is a facility factor, need an anti room to do typical isolation.
while the current infection does not warrant the isolation level-yet, just think about Ebola. -shoot me an email-bill2resist@gmail.com
step 1.
simple cheap device. for diy production. cheap – support for pro equipment
step 2.
new modules – attached to step 1 device. each module extend quality and function
step 3.
redesign based on real use step 1 and 2 and optimized for mass production.
TIME is a key.
People with the requisite medical knowledge and experience is the ultimate bottle neck in scaling up the availability of ICU beds numbers. Hack away at that problem.
https://onlinelibrary.wiley.com/doi/abs/10.1197/j.aem.2006.05.009?sid=nlm%3Apubmed
We’ll help. We’re a team of makers from Southwest Colorado. MakerLab @ the Powerhouse in Durango. We discussed this exact thing today before seeing this post. Any direction on if someone is taking lead on coordinating collective efforts? Seems like a design would need to be be replicatable quickly and easily. Also found this.
https://panvent.blogspot.com/?m=1
I‘m an engineer at Siemens Energy who builds low cost but high-end inspection robots for a living. I would also like to offer my expertise in construction and electronics to help with this project. Especially when it comes to 3D printable designs (masks, nozzles, adapters, casing, etc.). In my opinion, 3D printers are abundantly available pretty much everywhere and should be utilized where possible for that type of program. We need someone who will take the project lead here and who can define first work packages and the right teams to get started. We‘ll also need volunteers from every field, i.e. medical, intensive care, 3D design, fluid mechanics, electronics, purchasing, social media, etc. who don’t want to just post their opinions but want to get stuff done!
Here:
https://app.jogl.io/project/121
Hi Sterfan, lets talk about vents sometime, I am a Respiratory Therapist and Army-Navy Combat Medic, so I am used to working in the field. But I am not an engineer. I have a design I could use a hand inm -hope to hear from Granting Foundation on Monday. I could use a hand if possible.
I can help get things started by suggesting that we need to look not only at the vent itself but resources to operate it, most need 50 PSI air and oxygen, and all need 120V. which may not be available every where. so making it self contained would help, not a resource hog. Most of all needs reliability. so make it simple. My suggestion is, make a machine similar to the MA1, there are others out there- Birds and all, but every therapist knows the MA1 and how it works. We called them bomb proof.
they consist oif a bellows that controlls the volume-and needs to be precise, a controller motor to put that volume into the circuit-goes to the patient, and a means to mix gas to control oxygen. Probably need a means to control PEEP. the pressure left in the system between breaths. you will need alarms that dump pressure if exceeds a set limit-dont want to blow out a lung, and if we could add a means to do spontaneous breathing-great. will explain more if needed.
There are a lot of options for the circuit and exhalation valve, they are commercially available, but recommend using simple loop circuit with exhalation valve part of the vent, thats how they come now and thats how the circuits are made. several different ideas for the exhalation valve-most use a pneumatic valve that open and closes to all air to escape, but Servo uses a flexable tube that a metal arm pinchs off, sweet design and all,
let me know what you think, I can help a bit
Bill
https://www.instructables.com/id/The-Pandemic-Ventilator/
Here:
https://app.jogl.io/project/121
And besides factories making them, or ones that can be made at home, what if we get a design out to all the makerspaces and rally the Maker community to pump these things out. Everyone will be off work?
A week to design, a decade to get FDA approval, while trying to fight patent trolls.
Why not simply produce designs based on expired patents that were actually manufactured? I think ventilators predate 2003 by a considerable number of years. The requirements for the current crisis are not that ventilators of the absolute latest design are produced, but that functional ventilators for stricken patients can be produced rapidly. I’m not sure how much of a blocker FDA approval is going to be. Maybe it is, and we simply write off hundreds, thousands, or millions of lives in the name of compliance. Or maybe a suitable set of waivers can cover providers who turn to this technology. I don’t know the answer to that, but I am in agreement with others who advocate for open designs of tech in critical need.
Bubble CPAP (developed by my friend Jen Wung, MD at Columbia, Babies Hospital) https://www.indiamart.com/proddetail/fisher-and-paykel-bubble-cpap-18470469633.html
Its likely that in the event of a complete collapse, the death toll will be even greater.
I’d be going “Full Apollo 13” on this, to heck with the risk of getting sued.
In fact if they want to create thousands of “Prisoners of Conscience” when lives have been saved
then expect the biggest civil unrest in history.
I would actually willingly and proudly serve time if my actions saved dozens of people, what about you?
Hi, just a thought but could BMP085 or similar sensors be used?
I once made a BMP085 to needle converter using Polymorph for
an earlier experiment and it worked amazingly well!
Also re. hydrogen, pyrolytic graphite can indeed be used.
I did also come up with the idea of using high speed DC fans
originally used for PC cooling but they can be leverage for this
application. Locking together multiple small fans using the
existing speed controller is also viable though you’d need to
be aware of hygiene as others have mentioned
Re. medical ethics. If your design is sound then no-one is going
to criticize your actions. It is up to the individual doctors to decide
whether or not to use something that might help versus doing
nothing. The vast majority would hopefully vote with their
consciences and sort out the paperwork later.
So with an iron lung doing a PEEP(positive end expritory pressure) valve is less effective, that PEEP pressure with a vent is supposed to help force fluid back out of the alveoli into circulation. But at least you can get o2 sats up with the industrial oxygen and support breathing when the patient gets too tired using the iron lung.
I was reading the wikipedia article, a clay seal over the head and neck(probably the box joints too), wow that is seriously some stone age DIY, just need to be sure that the wet clay doesn’t drag down body temp. If iron-lunging a patient a nasal cannula or just an oxygen tent over the head should be enough, just have to get the ppO2 of the air up enough to get a good o2 sat and exchange enough air to prevent co2 acidosis. Still I cone form a world where you securely tube the trachea of anyone going unconscious, and paralyse them if we need that tube anyway(dont worry RSI we give something to sedate too, it blocks memory)
BTW in my service we did all BVM, for hours sometimes when bouncing out in the wilderness if the heli was unavailable, except the rare transports where we had a real vent and a nurse or RT. I understand that the iron lung went away and the surgically installed airway was for quality of life and mobility vs living or at least sleeping in a tube; it also obviously gives almost 100% airway control as well as constant immediate access to the patient.
I am certainly interested to follow this project!
I think we may have all lost sight of what this was all about. At least what I think it was about anyway. Come up with ideas to supplement the lack of mechanical ventilators in current hospitals. Dr. Bird was not daunted by the regulations of the day but saw a need and worked to fill it. (1) Having worked in the medical field for more years than I can remember there were times we had to make due with what we had. We used the PR2(2) as a ventilator, these were treatment machines, but would supply positive pressure ventilation in a pinch when we had no more MA1s.(3) My reference to super peep above was really accomplished bu submersing an exhalation hose in a trashcan filled with water. the depth of the hose in the water regulated the pressure.
I was doing some of the first helicopter portable vent transports early to mid 70s. This vent as far as I know was experimental. I have worked with iron lungs(4) and chest cuirass.(5) I also think the inventors of these were not worried about regulations in the initial stage of development.
So here is what we should do…stop thinking about killing patients with our ideas but saving their lives in a pandemic.
Let’s keep the ideas flowing and if something wonderful comes of it, then and only then we should worry about regulations etc.
Just my 22 cents worth
(1) https://en.wikipedia.org/wiki/Forrest_Bird
(2)https://www.hksccm.org/index.php/43-relax/medical-things-of-the-past/1086-still-remember-this-old-ventilator
(3)http://museum.aarc.org/gallery/early-icu-ventilators/
(4)https://amhistory.si.edu/polio/howpolio/ironlung.htm
(5)https://www.hayekmedical.com/clinicians
Just joining this most promising thread, and let’s hope our collective brain power can soften the impending crisis.
Disclaimer: I am a network and robotics engineer, and don’t know much about ventilators or their use. But I do know sensors, actuators, control systems, and what a reasonably-skilled maker could do.
So, if the problem statement is to provide, say 250000 mechanical ventilation machines to supplement the about 160000 that are currently available in US hospitals, here are some scenarios we could consider:
1) refurbish all the old ones in hospital storage rooms
2) raid the veterinary clinics, as I believe veterinary OR machines could be adapted to human use
3) modify the software in the fleet of bedside CPAP machines so they can be used for a subset of the patients
4) look into an open source project to 3D print an updated version of the “Army Emergency Respirator from Harry Diamond Labs in 1965. It is a block of plastic that apparently has a bi-stable fluid passage powered by the compressed gas entering it. It toggles between inhale and exhale modes. https://agentgallery.com/objects/rare-1965-prototype-harry-diamond-labs-respirator The cool thing about this design is its simplicity (no moving parts), and probable ease to 3D print
5) Improve the istructables vent with two valves and a bellows. https://www.instructables.com/id/The-Pandemic-Ventilator/
I think it could be build in volume using irrigation control valves (from Home Depot), and manifold pressure sensors (from Napa auto parts)
6) build up a bellows-pusher with a windshield wiper motor. This sounds primitive, but with the right sensors and control systems it could probably work
7) (if all else fails, and if we still have a quarter million patients in need): weld a 3RPM gearmotor to a 10′ length of pipe, and put a couple of dozen cams on it. You choose the number of cam lobes to approximate the prescribed Breaths per minute, and the cam lobe height for the tidal volume. The cams drive a bank of bellows, which drive a bunch of tubes, which go to a few dozen patients in a big ward. Very ugly, but probably a plan of last resort that could scale
Thanks for listening, and thinking . . . .
Here is a dumb-simple design. It essentially uses one of those manually operated Bag-Valve-Masks [ https://www.allmri.com/images/product_images/original_images/bild.jpg ] and puts it under a strap attached to a motor/spindle. To actuate the bag-valve-mask the motor runs, winds the spindle, and tightens the strap around the bag. There are photos included in the patent;
http://www.freepatentsonline.com/20190336713.pdf
Hi I love the enthusiasm,. but remember someone is counting on this thing to work, refurbishing old machine -most went to mexico or third world countries and being used still, too much liability to keep old outdated vents in US. If you were to try and make a new vent-look at a Purritan Bennet MA1 for a basis, is simple and reliable-does the basics, and probably enough out there to show its workings,
But remember that they need a circuit in order to work-and the MA1 had a valve on the circuit, so maybe have valve assembly on the vent itself, makes it easier to work with,
Heater and humidifiers are nice but we use HMEs now -so dont sweat that.
using a single vent on multiple patients-sounds good, but not really an option-too many things can go wrong. one patient comes off-all loose the ventilator.
your expertise would be in working control motors and what are called demand valves, and pressure sensors, thats what all the vents are using these days. But if still want to build a vent, stick to the basics, we can modify later with attachments. it needs to give a set volume in cc or L normally in the 500-700 cc range, at a set rate so many times per minute, usually 8-10 bbm. and a Oxygen % (FiO2) of around 40%. Probably should add Peep -5 cm, and would be nice to have a baseline flow, 10 L:/M
hope that helps
Bill
I’d love to help, but I’m an engineer who doesn’t believe in recreating the wheel. So I would need to know what good existing models do, what are we are trying to mimic. Ideally I’d like the full specs on an existing machine. And that would mean everything, from tube sizes to controls.
I’m fairly sure many of us could knock up a ‘ventilator’ tomorrow, but chances are most would be more dangerous than any virus.
So what we need is a FULL specification of the required machine?
How much air, how often. Does it require heating/cooling? Does it require additional inputs into the air stream (drugs? moisture?) etc. etc.
If given a full design model, that was not requiring any specialist parts, it would still take me many months (6 plus) before I could produce any acceptable units, let alone the quantity that what may be required.
Maybe the occasion will arise where we will need a a very rough and ready version of a basic ventilator? But we still need some kind of basic specification of what this unit does…
Again, I’m happy to help, but I need to know what I’m trying to do..
This is absolutely what is required now. As I have just posted, I think it will be easier to fix the limitations of existing ventilators that aerosolise outputs than come up with a new design. But first we need expert guidance on what we’re supposed to be hacking and the relevant specs.
HEY Vinny – I am with you on this one. I have been following this ventilator blog for a day now, and it is evident most here do not have any idea of how to manufacture a ventilator (or anything else) As soon as I hear 3-d printing… well..xxx -. I wonder how many “old” or broken ventilators are out there? Is there an aftermarket for used hospital equipment? parts and supplies? Surely someone,somewhere has a User Manual, or Service Manual for these machines. or if really lucky, a complete set of parts drawings and process sheets. . I would even steal a copy if I had to. I have a complete machine shop available and a local manufacturer of medical equipment (with a clean room and certifications) right here in Daytona Beach where I have lived forever. You can reach me at BuyRaceDayProducts@gmail.com
1) Many medical doctors are not technically minded. They are clever use all the tech but I am talking about taking things apart and knowing how they work.
2) If they contribute to this they may be worried about liability, being accused of spreading panic and being censured by their professional bodies.
3) This may be why in all these groups you are not seeing for an example an Intensivist laying down a simple basic minimum spec for a ventilator design.
Relatively basic designs exist for transport of patients and use by the military in crises that are powered by the compressed oxygen supply, use pneumatic logic to cycle between inspiration and exhalation phases and use a venturi to entrain air. Some do not meet all current requirements in terms of safety and failure alarms. Examples would be products by PneuPac, the original Draeger Oxylog, and the Bird Mk7 come to mind. If you are not too fussy about such regulatory details, they can perform the priority A task of actually ventilating a patient reasonably well.
I am not sure on this but hasn’t Mr T already declared that if any regulatory or legal issues are impeding any company from going ahead and making products for this crisis, do not worry about it and get moving? Think about using an existing basic stripped down design.
This UK company seem to have some ventilator designs, perhaps it’s a case of seeing if they will share, decentralise manufacturing to owners of various machinery/ 3D printers
https://breas.com/products/
I thought I would look at this blog and see where it was at, based on the Youtube video, And it is simple to see that most don’t know what they don’t know.
I am a Engineer a Machinist and own a manufacturing business, I’ve done days of research on a AC mode positive pressure ventilator system and the responses here are like watching monkeys try to figure out how to get a apple out of the tree.
Justin, Yes yes there are a lot of un helpful posts here. Seems a Bag Valve Mask could be a basic start for a DIY ventilator here is an MIT student project from 2010 that does that.
https://e-vent.mit.edu/wp-content/uploads/2020/03/DMD-2010-MIT-E-Vent.pdf
Hi Justin, please check this website. They have just achieve to certify it with spanish medical authorities. It is open source, with 2 designs, one for makers and another for mass line production.
https://www.oxygen.protofy.xyz
This is a very interesting solution …
On their website it says ‘We’re waiting for AEMPS validation.’
https://protofy.xyz/OxyGEN-IP/
If you have something that confirms that this device HAS been certified, Id be very interested to see that.
Hello Gary, the model I told you a few days ago already have been officially approved by the medical spanish agency more info about the model here: https://www.oxygen.protofy.xyz/home
There is 2 versions, one for makers and another for mass production.
Hi-I can answer a lot of your questions,I am a Respiratoryt Therapist and am designing my own ventilator .as far as current models, first most vent require 50 PSI air to operate-they are pneumatic driven, there are 2 types , pressure cycled or volume cycled, most vent used in hospitals are volume, they take a set volume and deliver it so many times a minute. Most shall we say are very delicate instruments-not too robust -the most basic machine is the MA1, I learned on that one, The machine now usually have a setting so they can breathe in addition to machine breaths, Called SIMV. The other less used is called Assist Controlled.
So what you want is a machine that can deliver a set pressure or volume, has a flow to allow patients to breath on their own, provide a baseline pressure-called PEEP, and deliver a mixed gas of oxygen.
The old system is like being a plumber with tubes and hoses going everywhere. the baby bird is a good example-but units are more computerized now and more delicate. watch a $30,000 vent get sidelined from a filter material getting into it. They require power-120 and air-oxygen supply. So in thgis case dont just look at the machine, look at the resources needed to operate it and the manpower needed to use it.
If still interested-drop me a line, I have some ideas, and I need an engineer. bill2resist@gmail.com
https://patents.google.com/patent/US8122883?oq=medical+ventilator
I’m looking through patents now to see what the required specs are.
What is desperately required is a what we in the DoD can a ‘Performance Specification’ which details WHAT a device should do rather than HOW a device should do it. This usually details the way in which the user will operate the device and any tolerances from an interface perspective. There are some real problems regarding the various stakeholders (doctors, patients, med-techs) and what specific knowledge each role has that drive device requirements. Doctors provide standard parameters to a certified med-tech and then the med-tech configures the machine. The med-tech doesn’t have the authority to prioritize functionality of a ventilator and a doctor has no clue how to operate a ventilator nor is he familiar with how the ventilator’s HMI is typically laid out. Finally, most hospital being subject to liability are ill-equipped to deal with products of degraded certification which is common in a crisis such as this. At a certain point, you don’t care about Certifications but just want something to keep you alive. The FDA has outright said,”an uncertified regulator is often worse than no ventilator.” All they care about is liability.
I have been researching these and here are a few useful links:
https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?CFRPart=868
https://www.govinfo.gov/content/pkg/CFR-2012-title21-vol8/pdf/CFR-2012-title21-vol8-sec868-2875.pdf
https://blog.arduino.cc/2020/03/17/designing-a-low-cost-open-source-ventilator-with-arduino/ (Forum)
Good Luck!
Eric, I agree.
3D printer is good to do some jobs, like replicate a plastic part with the same material and sterilizing that part. But not for everything, and it is too slow to 3D print, and some 3D printers use materials which produce toxic vapors, that is absolutely forbidden for a pneumonia patient. the part should not expel such vapors when is used as a part for the ventilator.
In a situation like the present, we need to use whatever is at hand, a piece of cooper pipe, maybe pvc. if nothing else.
adapt available valves is more practical than design an own model to take a long time to 3d print.
The wheel was invented over a hundred years ago a. Low tech a easy to build and operate. It is the iron lung.
This: https://archive.org/stream/PopularMechanics1952/Popular_Mechanics_01_1952#page/n259/mode/2up