
We are hearing so much in the news about shortages of personal protective equipment, or PPE, for healthcare workers. Factories are being asked to perform the impossible when it comes to production be the need is so real, so immediate, and so widespread.
The problem with rapid consumption of PPE is that once it has been exposed to infection, it’s contaminated and can’t be used again. Physically it may be fine, but it retains the capability to infect other people. If there were some way it could be effectively cleaned and decontaminated for re-use, it would reduce the strain on the supply chain and result in a greater availability of PPE for all those who require it.
This is the promise of Battelle’s Critical Care Decontamination System, a shipping-container-sized unit which has received approval from the FDA at break-neck speed.
Hydrogen Peroxide: It’s Not Just For Rockets
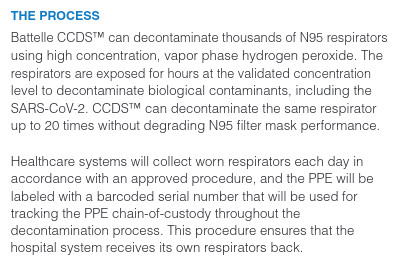
Each container houses a main chamber into which the infected PPE is loaded protected by an airlock and a set of filters, and the decontamination magic happens courtesy of several hours’ exposure to hydrogen peroxide vapour. The mechanism of using hydrogen peroxide as a disinfectant is simple and well-understood, it’s a chemical that readily degrades into highly reactive hydroxyl radicals which in turn attack any organic material they encounter. This effectively neutralises any viruses or bacteria that may be present on the PPE, leaving it clean and disinfected for its next user, and with the whole cycle from start to finish including loading and unloading taking twelve hours. The particularly flexible aspect of the system comes in its shipping container home, making it very straightforward to move from place to place where it is needed using standard trucks and loading equipment.
All this is most impressive and has the potential to be a game-changer for hard-pressed hospitals in the thick of the epidemic, but it is dangerous to latch onto any one solution and long-term the best solution will still be to build up a sustained manufacturing effort all PPE that is in short supply.
[Main image source: @PaigePfleger]













What about ultraviolet light? Seems like that would be less destructive.
Ultraviolet light has a hard time reaching much beyond the visible surface of an object. Render it rather useless for sterilization of air filters and the like.
But otherwise, it is indeed a way to make things sterile.
UV wouldn’t let you sterilize a pile of stuff, because only the outermost layer would be exposed to the light. So it would take up more room for a given number of items to be sterilized.
I would expect the hydrogen peroxide vapor must able to permeate through the cracks in a pile of stuck-together N95 masks so that all the surfaces are exposed to it. Perhaps it’s done at high pressure. Or maybe it’s like a tumble dryer.
Unfortunately the way the n95 masks work is through an electrostatic charge that captures viruses an particulates on the micron and submicron scale. A vapor bath of most kind would lessen this allowing for particulates to pass thru. UV (more specifically UV-c although UV-b would work) would not do this but like they say up needs to be direct.
maybe a little off topic, but years ago I worked on a beverage packaging machine line that used both UV light and hydrogen peroxide vapor together for sterilization. I don’t remember the chemical or microbiological reasons, but the combination of the two was much deadlier to bacteria than either one alone in any dosage.
We didn’t have shadow areas to worry about, but the UV did something to excite the H2O2, or something like that. (or maybe the atomized H2O2 did some kind of lensing for the UV. don’t remember.)
According to the EPA UV exposed hydrogen peroxides produce hydroxyl radicals (OH- with one electron stripped away) which is extremely reactive. I believe this is also one of the main principles behind “retrobrite” which is used to restore yellowed ABS plastic.
https://iaspub.epa.gov/tdb/pages/treatment/treatmentOverview.do?treatmentProcessId=-300168699
I wonder if hydrogen peroxide naturally has hydroxyl radicals as intermediate products, but just slower. I wasn’t able to find any information on this.
It does when it’s diluted with water I believe
VHP (vaporized hydrogen peroxide) is not that destructive to plastics and fibers, since it just reacts with the surface layer of the fibers. It can however oxidize metals fairly quickly. Usually we use steels 316L and better to prevent/minimize corrosion.
UV on the other hand can break chemical bonds of the plastic fibers. (that’s why initial experiments showed that the rubber bands of the masks deteriorated) Since UV cannot pentrate effectively after the first layer of fibers you will have to use a higher dose causing even more issues.
Overall if you compare the two solutions you will see more reliability issues with UV (due to shading) than you will see with VHP. Since this is a safety issue regarding high volumes of material reliability is key.
Note: Biopharma uses both technologies but prefers VHP for this exact reason
My hospital is using hydrogen peroxide steam sterilization for simple surgical face masks. I’ve seen your research ( and others) supporting this with N95 masks, but can’t find any research on the simple disposable masks. Can you advise?
Good luck finding UVC tubes anywhere for sale, factories are churning them out as fast as they can but demand is huge. We’re looking for some tubes in Europe for our UV disinfecting robot, none to be had without months of lead time.
Does a uvc led not exist?
I think they exist but are very low power and expensive.
Who could possibly know that one could just expose stuff to an immensely inhospitable environment, and have “clean stuff” as a result….
Viruses are’t really able to defend themselves much to begin with, considering that their normal thread out in nature is just bacteria literally eating them up…
Exposing viruses and bacteria to a high concentration of various industrial solvents tends to make things very sterile.
That this weren’t the practice to begin with is honestly a bit silly, though sterilizing things isn’t “free” nor cheap. So if it is simply cheaper to buy new PPE, than what it is to sterilize it, then why go for the later?
But with current shortages. Sterilization and reuse is fairly trivial. Unless one gets a shortage of applicable industrial solvents and the like.
I should probably add that there is a rather large difference between sterilization in a factory making PPE, and a hospital.
In the factory, it mostly contaminated with various oils, dirt/dust, and “normal” bacteria/viruses. Ie, nothing too bad to be fair, but sterilization is mostly to stop this from contaminating other things in the end application.
In a hospital, the PPE will most likely be contaminated with more hazardous stuff, making it a health hazard just to deal with it. So tossing it into a sealed bin and burning it is trivial thing, while sorting and re sterilizing it is a more fiddly process that risks infecting the person(s) dealing with the process.
>So if it is simply cheaper to buy new PPE, than what it is to sterilize it, then why go for the later?<
Well, from a training and practice perspective, if I don't absolutely know it's sterile, then it's NOT STERILE. AFAIK, in the U.S., all the med-training programs take that approach. For instance, if I am laying out materials for a sterile procedure, and I momentarily turn away from the prep area, letting it out of my sight, I am required by training, protocol and standard procedures, to assume it's no longer sterile, and have to discard and start again. If you're wondering how and why this approach has been adopted, it's based on all of the bad outcomes(infections, deaths, etc.) where someone "assumed" their materials were still sterile after a lapse in attention.
I do recognize we're in an extreme and exceptional situation where normal procedures may not hold…
Yes, ensuring that the tools one uses actually are sterile is an important part of ensuring that the patient doesn’t suffer other consequences down the road.
And one of the biggest reasons for why hospitals doesn’t re-sterilize their tools in house.
There is a list of things to consider.
1. Being the cleanup of the tools. (already needed)
2. Transport and sorting of the tools. (Some tools can use the same sterilization process, while others can’t. This is also where one risks infecting the person doing this job.)
3. The sterilization itself… (mostly a bit costly, and needs someone where it can be done.)
4. Repackaging the tools so that they remain sterile until they are needed again.
So just buying new tools that are already packaged properly is simply easier, cheaper and more reliable.
But it all depends on what one is trying to sterilize and what it will be used for, some things will be easier than others.
Surgical tools for an example will need other requirements compared to a pair of gloves used for swabbing the floor in the hospital lobby. And somewhere in between these two extremes we would find our air filter for the typical gas mask.
Google infection prevention checklist. Having a list of steps to follow whenever poking anything into a patient has dramatically reduced post-op infections.
It’s stunning how things that seem so incredibly simple have reduced infections and deaths. The Surgical Safety Checklist from the WHO which asks questions you’d think should be so obvious: what is the name of the patient, what procedure is the patient expecting, where is the patient expecting the procedure.
The implications of that subset of the checklist alone is terrifying.
I literally got up and walked out of a minor dermatologist surgery once, when the Dr. asked me what are we doing today? I was flabbergasted and went elsewhere.
CW – The point of the question was possibly to make sure you and the doctor were on the same page — They want to hear, in your own words, the surgery you are expecting. This both confirms that their patient data is correct, and that you understand what you’re consenting to. It doesn’t necessarily mean that the doc had no clue what the surgery was supposed to be — more likely that they wanted to confirm it with you as an additional safety measure. I had a surgery once where anaesthesia was required, and the surgeon used a marker to circle and sign the area of my body where the surgery was to take place prior to the surgery.
“But with current shortages. Sterilization and reuse is fairly trivial. Unless one gets a shortage of applicable industrial solvents and the like.”
Sterilization of something that’s intended as single-use is *not* trivial. What the article doesn’t mention is that the sterilization can only be done 20 times before the mask starts to physically degrade. If the process could be done like, 1000 times or something, then it’d be trivial: you just date the masks, sterilize them each day, and toss them after a year or so. Wouldn’t matter that you don’t have a perfect count of the number of times.
But when the limit is 20 times, the logistics become a *ton* more complicated. Now you really, really need to take care to make sure you’re tracking everything, and you need to inspect each of them to make sure that they aren’t damaged by use (outside of your sterilization) as well.
Now do all of this 80,000 times a day. I don’t even know if I could mark 80,000 masks with a sharpie in a day without going mad.
“which has received approval from the FDA at break-neck speed.”
To be clear, it received approval at “break-neck speed” after the governor of Battelle’s state (which also happens to be located in the capital city of the state, so literally right down the road from the governor’s office) publicly called them out for a half-assed approval and *directly called the President*. So… not exactly “break-neck speed,” more like “get this done or you’re fired.”
I only really meant the sterilization itself. The logistics and safety around it is a totally different can of worms.
But even if something only can be sterilized 20 times, that doesn’t make it all that much harder to track.
One solution is to label it with the date it were opened. And then expect that it will get circulated on a roughly daily basis for two weeks before you toss it away as junk. (that is only 14 reuses, so well within it’s useful life.)
Another solution is to add a strip of circles to it, so that each time it gets sterilized, you punch out one of the circles. Eventually, there is no circles left, and therefor it has reached its end of life. (of cores we can’t punch holes that renders the PPE useless, so use common sense and have it as a tag/label hanging from the item, like the label on most clothing…)
Yet another solution is to embed an RFID tag, but this is likely cost prohibitive in some areas, not to mention that it isn’t obvious how long the PPE has been reused, unless the end user scans the RFID tag.
When something is intended for single use, and 20 counts degrades it, that means you’ll need to inspect each of them to make sure they’re still usable, *in addition* to tracking them. These things weren’t meant to be reused. That’s not exactly something you can automate, which means humans. Which means now you also need to make sure your humans inspecting them stay sterile too. Which means the simple procedure gets a ton more complicated.
This isn’t me making things up, either, details on this are all in the original Battelle report from the FDA study several years ago.
Degradation of an item is usually linear or exponential in nature.
So the first couple of reuses will not have a major degradation, so no real need to thoroughly check for this.
Unless we have a process error during re-sterilization, so we should still take a few sample to check for such issues.
Otherwise, degradation isn’t a major issue, and one rather has to check for other issues, like things not being sterilized properly. But that our sampling procedure will also tell us.
It all though greatly depends on what the document means with “20 times without degradation”.
Maybe we for safety reasons needs to start tossing out items before that limit, or maybe an item twice over that limit is still okay 50% of the time. The document isn’t clear in this regard.
We could logically reason that 20 times would be the number of re-sterilizations we can go through while still being comfortably within our set requirements for the intended application.
Also, the people inspecting stuff wouldn’t need to even be remotely sterile, ever heard of a glove box? Then the main thing is to wear appropriate cloths as to not contaminate stuff with one’s hands, not to mention that one can set up a “basic” clean room. (Basic as in we don’t expect to perform surgery for a few hours in the room.)
Not to mention that final cleaning, inspection and sterilization can be performed in the glove box itself, before it gets repackaged.
These things have a working life of *1 use*. That’s their design. Which means that the failure rate basically should just be assumed to be random.
You can read the original Battelle paper on this – every single mask needs to be inspected to make sure that it *can* be sterilized and reused. The logistics of inspecting 80K masks/day alone are huge.
“Also, the people inspecting stuff wouldn’t need to even be remotely sterile, ever heard of a glove box? ”
Sterile is relative: obviously humans are never “absolutely” sterile while they’re alive. A glove box is just a way of making sure nothing from inside gets outside, and nothing outside gets inside. In other words, the inside stays sterile relative to the outside (and vice versa).
But again: we’re talking about *80,000 per day*. Now think about the logistics of pushing 80,000 things through a glove box. Way easier to put the humans in a hazmat suit.
>Degradation of an item is usually linear or exponential in nature.
In failure analysis, the probability of failure is expected to follow a “bathtub” curve. Some items will not survive the first re-use, while others won’t survive the 20th.
I wouldn’t be surprised if the masks often fail due to the rubber bands or ear loops or whatever breaking, or the metal nose strip becoming so bent that it becomes too hard to make it conform to your face, before they fail due to repeated sterilization. (Though perhaps that’s what you meant also.)
Which inspection model is likely to skip or miss a degraded unit : the one inspecting based on a low life expectancy, i.e. expectation of close attention, or the one with a really high life expectancy, i.e. oh it is probably still good?
Tracking the number of uses is equally important to both, so that doesn’t really matter unless the method is inefficient or prone to mistakes that allow complete bypass of the process.
Huh? It’s not equally important to both. If you’ve got something that can only survive 20 sterilizations, and one which can survive 1000 sterilizations, miscounting a use is 50 times more likely to result in a failure, so you need a counting process which is 50 times less likely to miss.
In fact, one of the benefits of a high-use count setup like that is you can *measure* how often you screw up, with a secondary system on a small number. Then you can just adjust for margin and now you know with a high degree of certainty how many failed cases will slip through (by projecting forward). You can’t *guarantee* you’ll never screw up.
With a low-use case situation, you can’t do that as easy, because you have no margin to give.
Based on all the information I’ve been able to read, it seems that a soak in water in a sous vide machine at 160F will be sufficient to kill SARS CoV-2 and make the N95 masks suitable for re-use.
Just because that would take care of SARS CoV-2 doesn’t mean it would be enough to sterilize a mask that was used in a hospital. Don’t forget, people don’t stop having every other disease when a pandemic hits.
And this is a large reason for why even re-sterilizing PPE and other medical equipment tends to be rather hard to begin with. Just handling it can be a health hazard in and off itself at times.
Not to mention all the legal responsibilities a hospital has about using sterilized tools to start with.
Agreed, but for people at home with limited N95 masks and the need or requirement to wear one when out (or in if they have a quarantined family member) the ability to re-use them is valuable.
But the mask itself might not survive. Adhesives might dissolve, etc.
Also you’d have to dry them. Otherwise the mask would be a damp home for microbes.
I tried it and the mask emerged unaffected. Drying was a simple matter of hanging it up for a bit. If you’d ever tie a handkerchief over your face, this would be no different, microbe-wise.
I also tried using the household oven on its lowest setting. It just doesn’t control temperature well enough. The mask deformed in some places and the elastic straps became fragile.
You cannot be sure that all the fibers remained intact and in place. masks are supposed to stop particles of 0.3 microns and larger, and if that capability were compromised by a sterilization technique, the results could be disastrous.
It’ll clear covid, but what about all the other microbes around the hospital?
This is definitely not intended for use at a hospital. Though maybe a soak in quat sanitizer followed by this treatment might be a good way to go. It is solely meant for home users to extend the life of their masks 10-fold or so.
The most practical way to decontaminate an N95 mask from coronavirus at home is to heat it in air to 70°C for 30 minutes. Do not immerse it in alcohol as this dissipates the static electric charge from the fibres. The method is explained by the inventor of modern spun polypropylene filter masks in this article:
https://utrf.tennessee.edu/information-faqs-performance-protection-sterilization-of-face-mask-materials/
YES, thank you for this! This is exactly what I was told by a friend who’s in charge of the ppe protocols at her clinic. She said that people had been using liquids (sanitizers, bleach solution, etc) at some hospitals and were effectively killing one of the filtering capabilities of the masks because the static charge was removed. I can envision a bunch of hackaday users’ home-made temp-controlled reflow ovens with hooks for hanging n95 masks.
I tried that, it is hard to find a well regulated, 70C environment. Home ovens are *not* good enough. Parts of the mask degraded/deformed and the elastic straps became fragile.
Use a lower temperature, but leave it in longer. It takes 3 days at 21-23 degrees. Use 30-40C instead to make it more thorough, but still leave it for a few days. Use a simple cabinet/box with a small heater like a few lightbulbs, or a heating pad.
Rotate through a few sets so the waiting time doesn’t interfere with work.
Oh the irony of banning higher wattage incandescent bulbs.
Hospital autoclaves work as well.
https://www.cbc.ca/news/canada/manitoba/manitoba-researchers-answer-shortage-n95-masks-1.5518226
For home use:
https://www.ncbi.nlm.nih.gov/pubmed/12267939
The Technical University of Delft recommended the following: 15 minutes at 121C using a sealed bag in a sterilisation machine will decontaminate an FFP2 mask upto 5 times, before it is rendered “ineffective”. Every hospital should have one, since it’s also used to sterilize equipment. Using radiation will render the mask useless.
I have to assume that the PPE can not take the heat of an autoclave or is not washable in a good hot detergent with chlorine or iodine.
Why not the systems used to irradiate food and sterilize things in-situ? I think they use either a strong gamma source like conbalt-60 or an electron accelerator and are continuous with a conveyor belt.
A lot of hospitals use UV light to sterilize rooms. All sorts of ideas that are NOT cost-effective because of red tape.
Ionizing radiation is a bad idea on something that must keep it’s electrostatic charge, as ionized gases (air in this case) are conductive.
The inventor of the electrostatic charging technology used in N95 masked did his own testing on different sterilization techniques. Dry heat, boiling in water for 3 minutes, and steaming all were effective and safe for the masks. UV wasn’t based on potentially breaking down the materials.
https://utrf.tennessee.edu/information-faqs-performance-protection-sterilization-of-face-mask-materials/
They came up with the overseeing body that approved it. Governments always contract out work like this anyway, so what difference does it make?
I don’t agree with your definition of socialist but besides that our current system is due to admitting no governmental control leads to chaos.
We are going to have a fun discussion when I get back from dodging surveillance drones.
You are thinking of chrony capitalism, basically government or kings/church handing out the licenses to make things, settling certain activities on guilds (unions), etc. Or Bismark Welfare State, the system that wrecked Sweden in the 1980’s. Or Fascism, where means of production are privately owned (a way to feed wealth to those in charge) but what is produced and how much is controlled by the government. Is is incredibly dangerous to flirt with any of these ideas because they fail quickly and lead to finding scapegoats and war.
I think younger Americans are drawn to a combination of chrony and Bismark.
From their website: “Battelle oversees more than 27,000 employees at eight national laboratories.”
The line between government and non-government is pretty fuzzy here. They’re a private non-profit with a lot of revenue from government contracts.
Are they the progeny of the Manhattan Project? Seems there is a continuity.
Only by association. Battelle is a charitable trust formed through the will of some rich guy (named battelle) in the 1920’s, if I remember right, who got very involved in R&D, specifically materials science, and at the same time somehow got involved in security, and because of the combo ended up as a primary contractor for most of the cold war nuke development and cleanup stuff. They are usually the people who show up to close down reactor accidents, like the whole Hanford site.
And all that radioactive waste from the Manhattan project is still lying around in corroding tanks and open ditches at Hanford.
The company with the Pentagon contract for surgical PPE would never let that happen. Much more profitable to make sure they keep buying new disposables.
Everybody blowing 1% peroxide through a vape and claiming they built a steriliser in 5.. 4.. 3..
i build an ozone chamber with a cheapo ozone generator tube where i put in all groceries and post i pick up for the neighbours for a few hours. To my understanding ozone should work just fine?
it should…just keep it away from people
BUT – it would make sense to actually test its efectiveness. Buy a bunch of pre-sterilised cultivation petri dishes and do “before” and “afrer” swabs, leaving some unused for control. If you can kill bacteria, you are definitely destroying the viruses.
https://youtu.be/2UdtKssU7po
(Tech Ingredients channel)
has a great explainer on how to build a ozone chamber
Very innovative! But here is the ultimate in PPE for you, please evaluate and disseminate this information as widely as possible.
The COVID-19 virus is, in abstraction, just a finite automata propagating through a substrate and that substrate is humanity, most mitigation efforts center around futile attempts to partition off parts of the substrate, other more effective but risky strategies involve modifying the behavior of the substrate to make it hostile to the virus. Great work guys but you got lost in the details and missed something very obvious.
Make humanity just a small part of the substrate and make most of it incapable of replicating the virus.
So how can we do that?
Genetically engineer a lactobacillus bacteria that is ubiquitous in the environment and on human mucosa so that the bacteria expresses the ACE2 (or any other required viral target!) gene so that the virus attempts to merge with the bacteria as if it was a human cell. The bacteria will however be engineered to immediately destroy the conserved parts of the viral genome. You can make the organism safer by also making it dependent on an artificial amino acid that does not exist in nature.
This lets you brew up a self replicating and sustaining, yet controllable, bioshield that can cover surfaces in buildings, public spaces and on the bodies of humans including the areas that are targeted by the virus, the mucosa.
NB this system can help protect against any virus that enters via the mucosal route, and it also prevents those already ill from shedding so many viral particles via that same route.
Pandemics always come from a virus that jumps species. You never know what they are going to do.
It’s really, *really* difficult to make an engineered bacterium that can compete with natural ones. They have a billion year head start on efficiency.
If a bacterium isn’t using a chunk of DNA to survive, like, if that chunk isn’t essential to its reproductive or metabolic success, it’ll quickly accumulate errors in the DNA, and fairly quickly end up just chucking that chunk of DNA, because the bacteria that reproduce the fastest outcompete all the others through sheer numbers so there’s a strong driving force to have the smallest genome as it replicates fastest. (Error accumulation is natural: conserved DNA sequences are conserved not because of repair, but because the ones with errors die.)
So to make a bacterium that lasts in a wild environment, with some novel DNA, you have to find a way to make that DNA critical, an improvement in reproductive success, and probably shorter than the existing wild-type bacteria. And it needs to have zero metabolic cost compared to wild-type.
Engineered bacteria work great in cultivated monocultures in industrial situations. I don’t think we’re anywhere near being able to design stuff that works in the wild.
Note to the above: you can improve DNA replication fidelity and DNA repair behavior. Eukaryotes have those functions. But they’re energetically expensive and take more DNA, so they can’t compete with bacteria that lack them and use sheer quantity to overwhelm the fancy ones with the fancy DNA repair proteins. Eukaryotes reproduce so slowly that we can carry a whole bunch of extra DNA for special situations like repairing busted DNA.
How about a bacteria that exists naturally in humans, modified to be a juicy ‘fly trap’ target for the virus, but with a flaw in its modifications to that after reproducing X number of generations it’s back to being identical to the original bacteria?
It’s hard to fool evolution. One of the problems with developing vaccines by damaging/attenuating them is that they often rapidly regain virulence through mutation. I was reading about people’s efforts to figure out which of the four genes that the corona virus’s RNA codes for does what. The way they did this is by cutting out bits of the RNA and trying to make it reproduce. What they find is that random mutation means it’ll somehow get those bits back and go right back to being its most pathogenic form. I was specifically interested in seeing if it would be possible to change the hinge mechanism in the S spike, so that after binding to a cell surface receptor, it had reduced ability to change conformation and force the viral lipid coat and the cell lipid coat into contact, causing them to fuse, and sure enough, someone had done exactly that, and it dramatically reduced the virus pathogenicity for a couple of generations, and then it was right back to its original form. Bacteria do the same thing, reversion to a stable form, only even faster because they have specific mechanisms for swapping DNA sequences with each other so they can try to juggle DNA and get back to running.
The way we test mutagenicity of chemicals, and characterize how likely they are to damage your DNA, is by using a variant of bacterium that has a mutation that removes its ability to metabolize a particular type of sugar. You plate it on agar that contains that type of sugar, and it’ll starve to death. You then plate it on that sugar and dose it with varying amounts of the chemical being tested, and if the chemical mutates the bacterium, one of the mutations will be the one that makes it randomly regain the ability to metabolize that sugar. So you have a whole bunch of plates, and each one you add 10x the concentration of chemical, and the ones where there are nice healthy bacterial colonies growing, show you the threshold at which that chemical, at that concentration, causes a known amount of DNA mutation. That’s how good bacteria are at reverting to wild-type and evicting designed mutations.
By the way, that’s also a beautiful demonstration of evolution. Our primary test for chemical damage to DNA only works because evolution exists.
Evolutionary amplification is spectacularly effective, and we don’t yet have the ability to beat it with engineering.
A bacteria sounds like massive overkill. Why not just make a protein that’s a juicy “fly trap” target for viruses that actually engulfs the thing and destroys it? I mean, literally like a Venus flytrap.
That sounds pretty good, right? And it’s extremely simple! Just a single protein.
Turns out it is. We call them antibodies. Problem is that nature is way, way better at making them than we are. If you *really* want to talk about using bioengineering to fight diseases, figure out how to make antibodies.
If people want to start reusing their surgical gloves I still have a tube of “liquid glove patch” for repairin surgical gloves, should they get a hole in them.
7 mil nitrile is pretty tough. I can reuse them multiple times doing resin casting.
>Factories are being asked to do the impossible
Does nobody know about wartime production pushes anymore? We can absolutely scale up production. The state just needs to give the go-ahead. We need to build hospitals, build ventilators, build PPE factories. We did much more challenging things than that in mere days during WWII. Why are we acting like everything’s impossible now? We’ve been wallowing in the knowledge economy too long, and now that everyone’s “working” from home it’s been laid bare that the vast majority of those industries are total bullshit.
Are we saying that we can build enough of these massive decontamination shipping containers and distribute them around the country–but somehow we can’t make a bunch more masks? What? Is this just a PR stunt or do they actually intend to produce enough of these to make a dent, because it seems like it would be more expedient in every way just to make tons of masks domestically.
It would be a MUCH needed stimulus for the economy. Instead of putting all our eggs in one basket and only isolating to stop disease transmission, we should be VASTLY increasing healthcare capacity–just in case our efforts aren’t enough. Spoiler: they won’t be. People don’t have the resources to shelter long enough to flatten the curve as much as we need to. And we have to flatten the hell out of it because our skeletonized healthcare system pretty much always hovers at full capacity without any pandemic at all. Big health intentionally keeps it that way to minimize waste and maximize profit. It’s horrendous. A few extra patients is all it takes to back up most hospitals. We need more, full stop. We can balance both strategies.
I’m floored that we can somehow manufacture prodigious numbers of war machines and munitions at a moment’s notice, but for some reason a few little breathing masks and glorified air humidifiers/pumps are somehow beyond the pale. We could do this. This is the USA. Why is this mostly being treated as a pipe dream? Let’s just make more so that even a terrible curve is manageable. We need backup plans in case the very naive “everybody in the world stay home for eighteen months” plan falls through–which IT ABSOLUTELY WILL. The authorities aren’t going to follow that through to completion when we start seeing 30% unemployment and The Great Depression 2.0. They just won’t. We need to face reality here. Maybe we could… y’know… have some domestic manufacturing again. Because millions of lives depend on it. This defeatism is deadly.
During WWII the US largely nationalized corporations. They said “Ford, you get no more steel unless you use it all for making tanks.” Current Administration says “we can’t guarantee that any vaccine produced will be affordable because that would reduce the profit incentive for companies to develop a vaccine.” https://www.statnews.com/2020/02/27/azar-coronavirus-affordable-trump/
If you actually want a wartime production push, you need an administration that acts like there’s a war on, not one that acts like the free market is going to invest billions now for a possible (well, inevitable, but not actually happening right now) future need.
US manufacturing (and, really, manufacturing everywhere) has completely embraced just-in-time processes. The whole point of JIT is reducing overhead. You can read ‘overhead’ as ‘buffer’ if you want. A JIT system is engineered to exactly match baseline demand, and as such, is catastrophically unable to react to a process that is out of control.
Even in WWII it took a couple of months to get a lot of stuff up to capacity. They were big things: ships, for instance. But we also had almost a year of pretty much knowing what was about to happen. We had designs for Victory Ships and tanks mostly ready to go, and some prototypes finished. (And even then there were issues, like victory ships cracking in half because the techniques used to speed up production resulted in previously-unknown manufacturing defects.)
JIT means “Just In Time”, and “SMED” means “Single Minute Exchange Of Die” which is a process for handling quick changeover, and Genki Genbatsu means going to the workplace to see how the work is being done and see if it can be improved to reduce waste and improve flow. Lean systems should actually be able to manage processes better, and optimize stuff better in realtime, if the situation is STABLE.
I’d put less blame on JIT, and WAY MORE on instability, and a lack of coordinated planning/process flow awareness and planning. JIT is more vulnerable to supply shocks than systems with a buffer, but buffers fail too (become outdated, reach end of life before use).
In the interest of national security, especially in regards to vital continuityof service issues, vital supply chains should have been better mapped out and evaluated for failpoints such as single foreign supplier, or red tape, or non-preferred (read last one served) client status. Some anti-trust legislation probably could have helped to keep a more diverse pool of suppliers in business that could have been drawn upon as well.
I think the problem here is
a) Nobody is sure how to adapt to what (superfluid situation with NO STABILITY, that is changing daily)
b) Nobody was visiting the different workplaces to coordinate stuff. That stored ventilator fiasco should NEVER have been allowed to happen. Equipment like that needed to have periodic checks to periodically re-qualify it. FEMA should have had regular warehouse inspection/quality tests. A healthcare stress test could also have been better mapped out as well.
c) The loss (and disregard for) competent expertise and institutional memory from this government was staggering. Why the hell was there no NATIONAL COORDINATION on health services and health purchases?
d) Very few businesses can ramp up their capacity to supply 10X normal output overnight (I’m guessing this out of my butt, but it looks like we are using a lot more masks/gloves/toilet paper than before). Shipping areas within companies might not be able to handle that, let alone the manufacturing floor. They will also NOT handle it altruistically/for free. Ramping up for significant demand requires planning, time & MONEY!!! Money to hire staff, money to buy equipment, money for materials, money to rent additional space or set up additional facilities.
This pandemic was identified early enough (thanks to China broadcasting all the data it had) for agencies to start making purchases and to redistribute already existing stockpiles while rebuilding a new one (like rotating the items on grocery shelves). No coordinated effort was made in the USA when a buffer needed to be built.
I’m amazed there isn’t a Dwarf Fortress or Sim city mod called pandemic preparedness sim where whole crowds of people get to videogame out the types of preparedness steps that are required to handle something like this. I want to see a micromanagement video game based on this Covid mess to see how stuff like this can be gamed out.
Ford at that time owned iron mines, coal mines, coke plants (for converting coal to coke), and steel foundries. Henry Ford believed in his company owning as much as possible of the total production process for producing automobiles. He failed miserably at rubber, because he didn’t bother to consult anyone who knew anything about rubber trees, or any sort of botany.
During the Korean War the government imposed steel rationing for automobile production. Manufacturer’s rations were assigned for a few years based on their prior year’s sales. Thus with Ford, Chrysler, and GM starting out with the highest sales, the annual forced reduction in the number of vehicles they were allowed to build was nowhere near as large a bite as it was for companies like Studebaker, Packard, Nash, Hudson, Kaiser and the others that had survived WW2 and returned to building vehicles. Hudson in particular could have sold a lot more cars, especially given how they crushed everyone else in NASCAR during the 1950’s, but they weren’t allowed to build as many as people wanted to buy.
Also, since Ford was still mining their own iron and making their own steel, I wouldn’t be surprised if Ford was providing steel under the table to Chrysler and GM.
Absolutely. When I was Weapons Officer on a Destroyer in the mid 1990s three of my four M2 .50 cal machine guns had been manufactured by Frigidaire in 1943. The problem now is that the US has outsourced so much of the supply chain including tooling and production of raw materials that it is hard to recover quickly. Hopefully we will re-think this.
The States with Certificate Of Need laws are finding out the cost of barring rural hospitals from investing in equipment they “don’t need” because the patients who do need such equipment can be transported to the big city hospitals. Hospitals whose board members also sit on the CON committees.
Nevermind patients die during ambulance rides to the life saving equipment located miles away when they would have lived if their small town hospital had been allowed to have a CT scanner, or an infant incubator, or a high risk pregnancy support room.
I happen to live in a State without CON laws and the small town hospital here has their own CT scanner, capable of up to 8 simultaneous “slices”. The single slice scanner it replaced was sold to a hospital in Africa that had no CT scanner. With CON laws it’s likely that patients needing a CT scan would have to travel up to 75 miles from here.
Yeah. It’s evil. Our healthcare needs to be nationalized; this system doesn’t and can’t work.
It needs the opposite. It needs government to get out of the way. Start by banning CON laws and regulations, which did precisely the opposite of their stated intentions to *reduce costs*.
If healthcare has to be private then can we at least ban for profit insurance? An entire multibillion dollar industry that exists solely to degrade the performance of the system is fucking suicidal.
Im surprised that no one has mentioned the hazard of handling concentrated hydrogen peroxide. It can be done but it adds a whole new set of problems all of its own.
I would go for some kind of irritation for sterilization. X-ray, neutrons or even UV light would probably work.
Since these PPEs aren’t washable, you would probably still end up throwing out large numbers of PPEs. For example when for example someones bleeds on it. People tend to get freaked out when hospital staff are walking around in blood stained aprons or what ever.
Pffft… it’s not rocket surgery… oh wait, oxidiser for rocket fuel plus medical stuff, okay it might be the one and only actual definition of that. :-D
I was thinking that too, I hope they park the container well away from any hospital buildings and definitely not in the underground car park. All it needs is a bit of static electricity from a load of plastic things rubbing together…
Relax, it’s not like it’s also packed with hydrocarbons…. oh wait.
Just melt them down and make more. Solves two problems.
Me myself was thinking not to wear this cheap ass masks, though they are lower in cost. In time of shortage I was thinking of some sort of scuba-dive-mask with are connected to a system that it make possible to connect to and clean air is passed to the diving mask. I think this things do not wear out and easier to sterilise by heating, steam or whatever. Perfect fit, maybe a little but more infrastructural work but since “new hospital” are build on the fly take this suggestion into account? Some trolley system with compressed air which stays in the room of COVID-patient is also possible? Luckily i don’t have to work in hospital and hope i can stay out these scary situation but i think my idea is worth taking into account when it comes to future hospital design. Personally I think these is a good wake up call and not the last pandemic event..
I hope some researcher, hospital-builder will read my suggestion and do something with it. I will focus on speaker hacks ;-)
Such an hacked mask, with custom 3D printed valves adapters, has been used in italian hospitals to cope with respirators shortage and save lives
https://it.businessinsider.com/isinnova-maschere-snorkeling-terapia-intensiva/
What about fogging with chlorine dioxide? That stuff is FDA approved for no-rinse wipedown of food preparation surfaces. It wipes out bacteria and fungi. Unlike chlorine bleach that only kills the growing fungus, mold, and mildew, chlorine dioxide fog kills the spores so that to regrow, a new spore supply has to be introduced. One brand of it is vital oxide. I’ve used it in a simple fogger to eliminate mold from crawlspaces. Amazing stuff, wood that was spotted all over with mold appeared clean after treatment, and years later there was still no mold regrowth. Got a bathroom that smells musty? Remove everything portable, open every cabinet and panel possible, then set up the fogger and shut the door for a couple of hours. Unplug the cord from outside (or use a mechanical AC switching timer) then let the fog settle. The vapor decomposes to non-toxic, non-corrosive stuff.
Dunno if it’ll do anything against viruses.
Has anyone researched the use of ozone to kill this virus? I’ve read that it is very effective with others. Destrucation is measured in seconds.
Proud of my state and govener for seeing this project past the red tape! OHIO
Imagine using the internet to rail about government intrusion in business.
A study on PPE sterilization options in case of shortage. Gamma rays irradiation seems the most effective
https://www.ecdc.europa.eu/sites/default/files/documents/Cloth-face-masks-in-case-shortage-surgical-masks-respirators2020-03-26.pdf
As an average hacker, this is much easier to do:
https://juju.inexacte.science/NoCorona/BoiteDecon.jpg
I have been trying to promote the idea of doing the same kind of sterilization using OZONE for about a month now. To date I can get one news organization, hospital, etc. to look into this. I even wrote my local hospital and suggest they do something similar using an outside trailer and an industrial ozone generator.
Does anyone know WHY ozone is not being used. I believe it would be cheaper and less complicated than this H202 Vaporization method, although I’m glad to see that SOMEONE is at least doing something similar, at least!
I also confuse, ozone had been use to sterilize room and kill SARS in 2003, ozone is very powerful sterilizer if we know how to eliminate the bad effect. I just put anything i bought, food, veggie, fruits, everything into big plactic bag, press it until no air inside, and just pump ozone gas. Tied it and wait for 30 minutes just to be sure, open it outdoor.
I apologize for not proof reading my previous entry. Several grammatical errors and I said Can when I meant to say Cannot in the second line.
ANYWAY, I actually see two other people here mentioned OZONE before me. I loved the idea of using Ozone to decontaminate groceries and packages entering the house, I’ll start doing that as I have an industrial ozone generator I needed to buy when I had a house fire 12 years ago. I’ve used it many times since then on smells, mold, etc. both in the house and in vehicles. I did a LOT of reading when I first ordered it, as you do need to be certain the room is contained with no cats, dogs, etc. inside it. Ozone will kill anything alive, including viruses.
Also, lots of CPAP users now have So Clean machines. They are nothing buy small ozone generators. I stick my P95 mask into the chamber with my CPAP head gear and clean them both together. Ozone is hard on rubber, but guess what, no rubber inside P95 masks made by 3M, so no issue. P95’s are basically a higher end version of N95 masks.
I know California has some laws against the use of Ozone, but the rest of the country could be doing this. I hope SOMEONE from the government will read this post and promote the idea further. Lots of Fire Restoration Companies across the country already have these machines, which aren’t that expensive to begin with, and could do these services for next to nothing, or maybe even for free as a public service. I’d be happy to do it for my local hospitals, but I realize there might be some regulation or quality control issues. I’d simply set it up in my covered trailer in their parking lot. All I would need would be a 120V extension cord. ANYONE, with any kind of experience using Ozone could set something like this up in a few hours.
In any case, I think it’s a READILY available solution that hospitals across the county could be using NOW! I have found no good way to promote the idea up to now, but maybe this site can help spread the message.
If anyone wants to discuss this idea with me further, please Email me at Jackyikes@aol.com.