
Aging in Place is a growing issue facing the world. As the population begins to live longer, healthier lives we need to continue developing assistive technologies that will facilitate independence and safe living long into our twilight years. That is the topic of this week’s Time for the Prize. Enter your idea for Aging in Place by starting a project on Hackaday.io and tagging it 2015HackadayPrize. Do this by next Monday and you’re in the running for this week’s awesome prizes.
What is Aging in Place?
I use the “define:” search term on Google all the time and for Aging in Place it turns up the Center for Disease Control’s definition:
“the ability to live in one’s own home and community safely, independently, and comfortably, regardless of age, income, or ability level.”
I love this definition. How easy is it to get behind the concept of better quality of life for all as we age? Still not getting the thought process flowing? After listing the prizes I’ll illustrate a couple of projects that will give you a good idea of what people are working on.
This Week’s Prizes
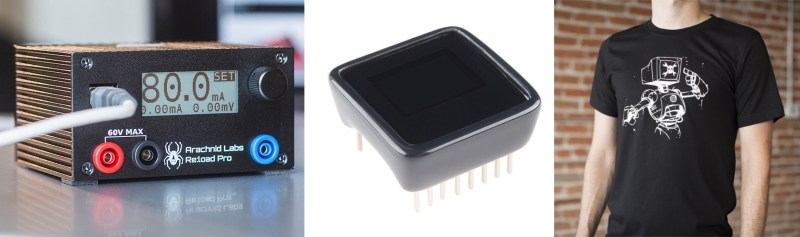
We’ll be picking three of the best ideas based on their potential to help alleviate a wide-ranging problem, the innovation shown by the concept, and its feasibility. First place will receive a RE:load Pro programmable constant current load. Second place will receive a Sparkfun Microview. Third place will receive a Hackaday CRT-android head tee.
Hacks that Help

 The easiest examples I can think of relate to medicine. A lot of the time people can be independent and high-functioning as long as they take the right medicine at the right time. The simplest way to ensure this is to use technology that helps track medication schedules. Pill reminders can monitor a pill case, sending reminders to you if you miss your schedule, and alertimg family or caretakers if you don’t respond to the reminder.
The easiest examples I can think of relate to medicine. A lot of the time people can be independent and high-functioning as long as they take the right medicine at the right time. The simplest way to ensure this is to use technology that helps track medication schedules. Pill reminders can monitor a pill case, sending reminders to you if you miss your schedule, and alertimg family or caretakers if you don’t respond to the reminder.
We’ve also seen technology built right into the cap of the prescription bottle. These caps have a timer that resets to zero every time the bottle is opened. But anyone who has taken several medicines on different time schedules can tell you that this can still be very confusing. We wonder if anyone can prototype a system that would use computer vision to verify and log the pills each time you take them?
Of course the prescription reminders are just one of a multitude of low-hanging fruit. Safety is another aspect. Here’s an entry that seeks to give peace of mind that the stove is off for those dealing with Alzheimer’s or memory issues.
Now you see what we’re getting at. What ideas do you have that can move the goal of Aging in Place forward?












I like the timer bottle caps, could be useful for people who want to make sure the cleaning people /grandkids are not stealing your prescriptions.
I think the timer bottle caps could be useful for anyone who takes tablets, Im not classed as elderly yet, but I do have something I have to take tablets to a routine to manage, and quite often I get distracted in the routine by the bustle of life and have to sit down and decide if I took the tablets already or to skip because Im not sure.
Also if it knew how many tables it contained (loaded with a standard amount then decreased by the dosage every time the lid is removed?) that would also be a great help. Little reminder about you having to get a renewal a week in advance would be great. The amount of times I have ran out on a friday night when I thought I had another week is shocking. Maybe I am shocking at managing meds, but I am not the only one…
There are the little pil cases you preload for the week, but I am not retired, and I dont really have time to do that.
Just thoughts.
I’m with you on all of this. Finding an eloquent, intuitive way to offload this record-keeping/reminder task would be awesome and to me it seems like exactly the type of things computers (electronics) are good at.
Imagine this, a standardized cartridge that your pharmacist would load with your prescription, and program it with the doctors order. You plug it into a standard machine that reads the orders, manages your reminders (including when a refill is needed) and dispenses on command. Such a system could also be voice or touch activated for the blind.
Even beyond simple stuff such a system could also help document usage for those with drug contracts.
A simple bar code system would probably be enough to start this. I can’t imagine that the schedule for drugs would normally be that complicated that we’d need more than a couple dozen bytes at most to encode the information.
Ask someone on cancer meds, or HIV treatments.
And sadly, most of those can’t be compounded.
Although I am surprised most people on multiple meds don’t take advantage of compounding.
Crush, blend, recapsulate. One pill per schedule.
There are some prisons that do something like this already. Obviously it’s not quite voice or touch activated, but the prison pharmacy receives an order, the pills/meds are put into a sealed container, and the container arrives at the prison where it’s distributed to the prisoner.
Obviously people who are aging in place aren’t prisoners, but there could be something you could use.
yeah.. the more pills one has to take, on varying schedules, the harder it gets to prep the next day/week’s worth of tablets.
It makes me think of the change machines, where a stack of tablets are loaded into a tube. Several tubes snap together. Once set, it vibrates/Berks on schedule. You grab and push a button, and the tabs are kicked out.
Won’t dispense off schedule so caretaker pill theft can only happen at the bottle. Compact enough to fit in a handbag or pocket.
For real forgetful people could be decorative and worn around the neck.
Would be best if it was similar in form factor to a smart phone.
Berks = beeps
Silly android. Wtf is a Berk??
http://cdn.meme.am/instances/57892159.jpg
A Berk is a sandal often worn with stockings, hence Birkenstock. B^)
Berk is Cockney rhyming slang for ‘c***’ (Berkshire Hunt)
There are pharmaccys that will put your medication i blister packs, so you can tell if yo had taken your meds or nit. The downside is that they are in blister packs. You ain’t got time to load a med box now? Man you are going to be screwed when you retire,if you think you will have time then.
Yup, I have a routine when I get up, involving taking the necessary tablets. If I don’t do it, an hour or so into the day I’ve no idea if I’ve taken them or not. Taking pills isn’t a very memorable experience, so no wonder it’s easy to forget doing.
I have an entire arsenal of these tools thought out and planned — my grandmother had a stroke at age 72 and lived on until 84 and needed significant assistance. She was not the only person in this situation.
1) Positive Pill Minder — electronically monitors the pills, creates the correct packet of pills and distributes to the user on time. Requests refills automatically.
2) PT Minder — goes to PT with you, records your PT session, uses Internet connectivity to parse what the therapist prescribes in terms of at-home PT. Shows on its screen how to do the exercises when it reminds you to do them.
3) In-home urinalysis kit — literally, it lives in the toilet. IoT compatible.
4) Dementia Minder – MCU-driven device that monitors your behaviors when at home. If your behavior or speech goes sideways, it will notify the physician, sending the recording of whatever unusual behavior it notices.
These are the four I remember from my journal. IIRC I have conceived of 12 of these, some of which are easy with today’s technology and some of which are hard or expensive. I would *love* to work for a company developing these things.
I love these ideas. You should enter them! You can make multiples entries as long as you post them as separate projects.
#3 is something the Japanese already have, or pretty damn close to it anyways. Last I read, the damn thing was mad expensive though. It’s called a Toto Smart Toilet.
Cheaper version of that would obviously be nice.
And what about the Sh*tBit?
On this page is an error http://hackaday.io/prize/details “Start your idea storm. Just talking about interesting problems and possible solutions could land you a small prize. Post your own project on Hackaday.io and add the tag “HackadayPrize” ” (ie, not 2015)
The pill dispenser needs to be a oversized glorified automatic pet feeder. The pills are placed in separate hoppers, the “feeder” is programmed with the type, quantity, dosage, etc (by the caretaker). At the appropriate times, a light and buzzer goes off and the correct pills from all the hoppers are dispensed into a disposable plastic cup. If the pills aren’t removed, the buzzer goes off again. If the pills still aren’t removed, a text message is sent to a caretaker. For the stubborn elderly, there could be a webcam that takes a picture of the user actually taking the pills. This would solve the problem of forgetting, of stolen pills (the unit would be locked), of running out of pills (the dispenser could email refill requests as needed), of incorrect dosage (to few or too many), of incorrect schedule, and of verifying the pill were taken by the correct person (with the web cam option). None of this technology is hard, and even a multi-hopper unit wouldn’t be all that expensive.
And when you drop and lose a pill, then the darned box is locked and you can’t get a replacement?
It’s designed to stop you forgetting to take pills, not to stop you taking extra ones. Just have a button that says “Missed pill”. You’d still know whether you’d had your days pill or not. You’d only press the “missed” button right after losing your pill. Assuming you can keep your memory together for 10 minutes or so, that’d be fine. Just in case, it’ll make a log that you took an extra one. If that turns into a problem, your carer will be notified.
It depends how much of your mind’s still left. Beyond a certain point there’s no point developing technology, you need proper full-time care. This is just to help people who are a bit forgetful, IMO. Forgetting your pills is a problem for lots of people.
Imagine the PillPopper a dispenser for scrip and regular pills using a vending machine mode. Either secure and monitored or simple non electric pushbutton vending.
Unscrewing and rescrewing lids times the number of items is a nuisance at least.
Pop pop pop! Pills in a cup.
Hoppers would need different sized ports or changeable ports to let only one pill out. Loaded tubes would be most reliable but need to be filled.
So, if we already have our project up but can think of simple things to change to make it more “Aging in place” friendly, how do we let you know? Or will all projects be reviewed again for this prize?
Reblogged this on Übermüdet Mirror and commented:
Bis wir alle unsterblich sind sorgt Hackaday dafür dass wir es im Alter leichter haben.
Go Hack
Maybe this is the wrong thing to say. I guess I come from a different mindset of people. If I can’t take pills for myself, and it gets to the point I forget my own name, or everyone around me, someone please go get the shotgun. I personally wouldn’t be able to make that decision when someone else is taking care of me, so I’m telling my family to euthanize my ass when I’m crapping on myself and talking to the people in the room that aren’t really there. I don’t see how that’s quality of life. It tarnishes the memory of that person. I hope nobody takes offense to it, if you are caring for someone. I would imagine they felt the same way at a younger age… But now they can’t tell if the sun is up or down at night.
Now as far as enhancing life at near elder level, I can understand how these devices could help extend your golden years, so instead of a good 15 years of focus and clarity, you might get 20. But there comes a time when it’s fair to them to let the earth take them back.
Please don’t read this comment if you are recently, imminently or inevitably* as it is critical of widely held beliefs on this issue.
This is based on personal and professional experience including palliative care and more extensively working with children with either incurable or curable-but-missed** diagnoses and often devastating morbidity.
This is opinion, and expanding on the thoughts above
Biggest issue with “aging in place” is we’re just not very good at letting our loved ones get on with it. Where the ethos is intended to be maintaining quality of life through maintaining community, family and place connections, it is more inevitably funded as a way of reducing aged care costs or shortening waiting lists.
And when we do achieve long-term care in the home (whether child or adult) We (including me) are very poor at choosing what care we do provide.
This is tied up with many of the difficulties of aging in place and effective palliation. It is often the cause of many of the issues detailed in the article, not least of which is the pills driving profits, often demanded by families, and to the dubious benefit of the patients (and families, physicians, and nurses and everyone else who takes on the burden of supply, cost and administration).
Don’t believe me? Riddle me these thoughts
– why are people over 80 treated with drugs like statins and clopidogrel (which take up the number 1 and 2 slots for drug expenditure in most developed countries) when we probably need to treat hundreds or thousand to change the life of one? (And we will never be able to do a good study to find out)
– Why is anyone above the age of 80 or so on blood pressure lowering medication, statins or anticoagulants when not Symotomatic
– why do we wait until we have to make a life or death decision before we have a life or death discussion?
– Why do our medical professionals have such difficulties in denying futile care when families just want “everything to be done”
– Why do we ask grieving people permission to withdraw care – akin to asking for their approval of death
– Why do we not understand that modern medicine’s version of “everything” involves pain, humiliation, grotesque procedures with outcomes that are often either unpredictable at the outset or inevitably complicated by loss of brain tissue
– why do we think that everything is curable when the reality is more that everything is open to compromise
-why do we think that medical complications are primarily the responsibility of the treating team and not the underlying illness
– why do we hate and complain to standards boards about doctors who tell us their understanding of the truth, especially when later facts find them wrong (whether the patient benefited or was harmed) or the outcome is poor
– and why do we assume that the second (third, fifth) opinion is more likely to be correct than the first – moreso when those latter opinions are more positive, offer therapy (proven or not, and rarely offering to fund it) or are more conforming to our own understanding and expectations
– What level of disability are we prepared to inflict or prolong on our loved ones who no longer have a say, because we fear death
– why do we fear death when most of us believe we (and usually our loved ones) will go to an afterlife and rejoin our family and friends there
– Why do we have such faith in modern medicine, when the evidence that drives modern medicine is denied flatly by politicians, pundits and people
– particularly when it has the poorest acceptance for those with the widest community benefits (children, workers, preventative and environmental health – toilets and clean water, female education, immunisation) but greatest expectations of those whose benefits are most expensive and narrow (intensive care, etc,)
– Why do we allow companies to demonstrate their drugs have a survival effect in the short term, but not show that long term use is superior to cessation? Especially in the age groups it ends up being used in, rather than the ones that show most effect
So in short how would I hack aging in place?
I would rephrase it as dignified dying in domicile, and ask all patients and family members to be informed to the point of comprehension of what intervention actually involves, and what death and organ donation mean to all parties; what their goals and thresholds are, and what they can and can’t expect of each other.
Ageing in place is a therapeutic strategy that inevitably shifts the balance of care away from consolidated providers and onto the patient and family. If we are to ask that of them, we should be frank with each other about what is achievable, what is futile or of unknown benefit, and what is inevitable*
* Technically death is probably inevitable. You can move to the Isle of Man, but you’ll still die there. Except if you’re a certain jellyfish.
** Not negligently, just rare-disease-common-vague-symptom territory
^ Warfarin and aspirin do not and never have “thinned the blood” and the viscosity of your blood is primarily determined by the amount of blood cells in it (generally measured by the amount of Haemoglobin, the oxygen-carrying protein package in red cells. The more Hb per mL, the more volume taken up by the carrying red cells and the more viscous. White cells can also have an effect in some leukaemias)
Warfarin poisons your liver’s ability to make proteins that normally coagulate (congeal) blood if exposed to certain stimuli; including things like “I’m not in a blood vessel” “Metal WTF?” “I’m surrounded by pus” “I’ve been sitting in the leg for a while now and it’s not moving – maybe it’s been bitten/frozen/paralysed” (DVT) “the wall of this tube/bunch of little yellow cells is telling me it’s leaking” – the latter being important if the vessel is sewn together out of goretex, cadaver tissue, the former pouch your heart sits in or the thing that gives you one of the three pulses in your wrist.
aspirin poisons the platelets ability to signal effectively. This means the usual coordinated response is much more disorganised. Think of all your scouting units losing communication.
That’s very long, but I think the point of statins is that they’re so cheap, it works out economical to give them to everyone for the help they give. They don’t have many negative side-effects. They’re also well off-patent so they’re hardly making anyone a fortune. Tho that depends on where you buy your drugs, and is open to corruption, but then that’s corruption that would be the problem.
Short answer, get yourself a national health service. In countries that have them, almost nobody would give them up.
Amen that, but we can always do better – and public healthcare has even more need to be ruthlessin it’s evidence base- we’re talking lives, not profits
Regarding statins, although atorvastation and sings statin are off patent, you will find many are on in-patent products costing nearly 10x as much as generic alternatives.
http://www.ncbi.nlm.nih.gov/m/pubmed/22392823/
(BTW if you’re worried about generics, don’t be. Even the counterfeiters know to copy the $1400 statin, not the $140 bio equivalent generic. Developing countries, however, are different)
The next issue is who is using it, and what is the number needed to treat. Obviously the higher risk you are the more likely the drug will save your life; but even in patients with 30% chance of CVS in the next year, the cost becomes significant
Even at 30%, treating for 10 years you will stood average 1 event in 8 people; and there will still be 2 or so events.
And we get treated at much lower risks than that.
Unfortunately even generic statins aren’t “cheap” – Aspirin is 20-40x cheaper, has a similar safety profile, and has similar efficacy.
But none of this helps if your all-cause mortality over 10 years is >50% because not enough people will live long enough for the statistics to show benefit.
http://www.medicine.ox.ac.uk/bandolier/booth/cardiac/statecon.html
My take, after nursing my wife through 7 years of a terminal illness is that at some point, prolonging life morphs into abuse.
Fuck that, I’m gettting every nanosecond I can. There’s absolutely plenty of time for me to be dead in. No point throwing away even my most basic cellular metabolism, it’s not like I get a second one. I imagine senility’s something I’ll quite like, I’ve had a bit of practice. Warm and worry-free. And even if I don’t, I’m sure I’ll forget that soon enough.
The world can afford to take care of it’s elderly. It’s just that some people have as much money as everybody else put together. You may have heard this.
The timer cap is very good idea but I see no way to setup an alarm ?
I’ve submitted my random idea for “tracking” movement of old peoples in their homes, should the movement stop, deviate from their normal routine then next of kin/carer is notified to check up on them.
Already did it a few years ago for my own grand’ma especially for bathroom with IR movement detection and also to check if she got nervous and move around too much in the house (Alzeihmer)
then you should have submitted it as an idea ;)
I also added awake alarm that warn me if she stay too long in the bed in the morning (may be seek … or worst…)
https://hackaday.io/project/5098-litehouse
possibly not as elaborate as your original concept…
A big problem I have seen more than once, is where the elderly person OWNS their own home, and their descendents use the first sign of “dementia” to stick them in a nursing home (where they rarely last more than a half year before losing their will to live). Then the paid for home gets sold quickly to get free cash for the descendents. Sadly, the antiques are often sold in bulk to a dealer at a fraction of the true value, again for quick cash. Will are rarely honored if a child can convince grandma to make them executor of the estate. So really, will these devices be allowed if the kids can gain control of the homestead in order to “protect grandma”? Yes, I have personally witnessed this, where I am convinced “grandma” could have lived for decades in HER OWN HOME that she knew well, if perhaps she had a live-in assistance (adult grandchild, perhaps) to keep her company and give her somebody besides herself to care for (or at the very least, a pet to care for, but a descendant would be much better). Devices alone are not enough, unless they have real “personality”, perhaps… They key is to have a REASON to keep getting out of bed, despite accumulating aches and pains… IMHO
In your scenario doesn’t reflect how the real world works. Nursing homes recoup the cost of care whenever they can, meany a greedy family isn’t likely to see any proceeds from the sales of a home and other possessions. The earlier they commit a parent to a nursing home, the higher the accumulated costs, the less for the family after the sales. For a person to get nursing home care at no cost. They truly need such care and are truly indigent.