In a perfect futuristic world you have pre-emptive 3D scans of your specific anatomy. They’d be useful to compare changes in your body over time, and to have a pristine blueprint to aid in the event of a catastrophe. As with all futuristic worlds there are some problems with actually getting there. The risks may outweigh the rewards, and cost is an issue, but having 3D imaging of a sick body’s anatomy does have some real benefits. Take a journey with me down the rabbit hole of 3D technology and Gray’s Anatomy.
It’s really simple to come up with a laundry list of how adding 3D scanning to medical procedures isn’t feasible. It would add a huge amount of expense in the form of equipment, personnel, and training. But I would wager the same arguments came up when first introducing MRI technology and look where we are with that now. Most neurological problems include Magnetic Resonance Imaging (MRI) as a diagnostic tool. For ailments where MRI is not ideal, the CT scan is used, and even more widespread is the use of ultrasound imaging technology. It’s worth looking at some of the highly touted emerging medical tech to see if we can figure out where it’s leading us. So if money and manpower weren’t issues, what role would 3D scanning play in healthcare?
My Teeth and Your 3D Printed Cast
I jumped on this magic carpet ride after seeing several instances where 3D printed casts were being heralded as the new hotness. They are tailored for the patient’s limb, impervious to water, allow the skin to breathe, and can be designed with Low Intensity Pulsed Ultra Sonic (LIPUS) modules which clip into the cast’s structure to speed healing. Here we see the Osteoid Medical Cast which includes those ultrasonic elements, and the Cortex Exoskeleton, but there are other non-arm examples like the ZDRAVPRINT.


The LIPUS has been through clinical trials, but the 3D printed casts themselves have not. A little bit of interesting design sure makes it look futuristic and that never hurts in selling an idea, however
In thinking about a 3D printed cast, I wondered where they got the model for the cast. How do you know what the arm is supposed to look like when the bone is set and the swelling is gone? The answer is that they don’t. The x-ray of the bone, and a 3D scan of the currently broken (and undoubtedly swollen) arm are used to make the model. In other words, this is medically quite similar to wrapping plaster and bandages around the swollen arm after setting the bone. Hygienically it should be better since plaster and bandage can soak up moisture and get nasty — and all 3D printed cast companies are touting that fact as loudly as possible.
It was at this point that I thought about my teeth, which are hanging out in a box in my basement right now. As a brass playing musician it concerns me that I might get in an accident and knock my teeth out. So I had a cast made of them. The idea is that I can take this along to an emergency dental visit and the dentist will use it to put my pearly whites back exactly as they were before the trauma. Could this work for bones as well? Maybe.

But in keeping with the analogy of teeth, for simple breaks it may be possible to design progressive casts that take into account the original state of your broken limb, and its current broken positioning. This is similar to how Invisalign dental braces work. Unfortunately doesn’t help my argument for pre-emptive 3D scanning. In the case of invisalign, your teeth are modeled in naturally crooked orientation, then straightened by the computer. If progressive 3D printed arm braces are only going to work for simple breaks, there’s no need for a starting 3D model.
Advanced Imaging and 3D Tools
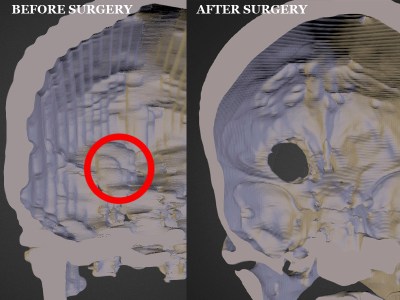 Pivoting away from casts, imaging technology has long been the cutting edge in medicine. The machines themselves produce fantastic data, and we’ve seen examples of how using this data to assemble 3D models is hugely beneficial. For instance, there’s a fascinating story of a brain tumor treatment greatly aided by an enthusiast’s 3D modeling skills. The data sets from the scans were rendered in 3D by the patient’s Husband to find the tumor hadn’t grown as rapidly as had been thought from a second MRI. These models were then used to print a physical model for planning the surgery.
Pivoting away from casts, imaging technology has long been the cutting edge in medicine. The machines themselves produce fantastic data, and we’ve seen examples of how using this data to assemble 3D models is hugely beneficial. For instance, there’s a fascinating story of a brain tumor treatment greatly aided by an enthusiast’s 3D modeling skills. The data sets from the scans were rendered in 3D by the patient’s Husband to find the tumor hadn’t grown as rapidly as had been thought from a second MRI. These models were then used to print a physical model for planning the surgery.
A less concrete example is this pencil cup. It’s a highly accurate model of a man’s face based off of CT scan data. Obviously there’s nothing revolutionary about printing 3D models with low-resolution plastic printers. But the parsing, assembling, and visualizing of the data speaks volumes. It should be noted that Computer Tomography scanning uses X-rays, and it’s almost impossible to argue that exposure is warranted in preventive cases. MRI technology doesn’t pose the same risk.
If we make scanning data like this available, and encourage people to come up with interesting uses for it, the next breakthrough could happen in a hackerspace, basement, garage, or on the couch while Big Brother drones along in the background. Considering how the general public reacted regarding privacy issue with TSA backscatter radar, making public high-resolution scans of people’s bodies isn’t going to happen soon, if ever. But it is tempting to think about the potential of crowd-sourcing medical scanning research.
Unintended “Side Effects”
 Even if we could find a great reason to image our bodies on a regular basis, it still can do more harm than good. One example is over-diagnosis. If you are scanned and examined regularly it increases the odds that some ailment will be found, and that includes false positives.
Even if we could find a great reason to image our bodies on a regular basis, it still can do more harm than good. One example is over-diagnosis. If you are scanned and examined regularly it increases the odds that some ailment will be found, and that includes false positives.
I found this Science Friday discussion to be very informative. There is an incentive for companies that make scanning hardware like MRI machines to encourage scanning as preventative medicine. But this drives up costs and increases over-diagnosis.
The solution is to take the NSA approach to full-body scanning. You collect the data but you don’t look at it. The scans only get pulled out when “trying to put Humpty Dumpty together again”. You could simply walk down to your neighborhood 3D scanning booth and have yourself MRI’d. Unfortunately this tech costs around $3M new and is unlikely to come down in cost.
The popularity of 3D printing has the power to revolutionize all realms of technology. But so far I’m still searching for the route that allows it to take widespread hold of how we repair our bodies and help them last longer. If you have a gut feeling of where this is all going, I’d love to hear about it in the comments below.













My local mall has full-body 3D scanners in the main hallway where small carts/stalls are setup. They are big enough to fit about 3 people into, if you want a scan of you and your friends/family.
Which mall/city/country?
I found this Forbes article. And, I remember a few years ago of a startup that partnered with several stores in the mall to do a 3D scan of customers for a few bucks, and spit out a list of what clothing items in what sizes would fit a customer. Can’t recall who or where, though.
http://www.forbes.com/sites/jenniferhicks/2011/10/24/bodymetrics-creates-3d-body-scanner-for-new-look/
New free app for same thing : http://www.nettelo.com.- https://www.youtube.com/watch?v=nvSV5YX0h5Q
doesn’t answer broken bones problem, but body tracking (pregnancy/gym.diet ) and size recommandation on their way into this app.
Washington Square Mall here in Portland, OR… there’s a map of their locations here:
https://shapify.me/scanning-point
Yes where at, because I’d love to mess with that a bit.
Talking of future tech applications, I was wondering if anyone knew i there existed such a thing as a programmable breadboard? one that didn’t need jump leads that you could programme to build the traces inside through a series of gates? I have been trying to find one, If it has not been invented yet I might just have to try…
No, because it would be much more expensive and restrictive that hobbyists would accept, and wire is cheap.
It all depends on what you want to do. If you want to experiment with just a few discretes, a breadboard is still the best option. But if you want to do more complicated analog or digital signal chain stuff, then FPGAs or mixed signal arrays like PSoC where all the components you might need are integrated in one chip would be better.
Hey thanks for the info, I haven’t really looked at FPGAs, I have heard of them just didn’t really know much about then. I just thought breadboards are a bit messy when you need a lot of components. wires everywhere and having to search for a wire that isn’t connected properly isn’t much fun.
That’s why modular dev board systems like Arduino shields and Raspberry Pi hats are popular. They take popular combinations of components and stick them into tested and documented modules that you can combine with minimal frustration.
Want to make a sous vide controller? Buy an Arduino, a relay shield, a thermocouple shield, and a touch screen shield and just plug them together. Change that to Arduino, GSM shield, and GPS shield instead. After that it’s all a matter of writing glue code connecting existing libraries.
Many here argue that this is “cheating” or “noobish”, but that’s just the elitism talking. You will miss some of the low-level stuff that you would get from wiring together components or doing signal processing in the analog domain, but you will get your project done. Likely your feeling of accomplishment will encourage you to explore the fine details. For that, breadboards will still be around as learning tools.
Thanks, I have used some arduino sheilds and wanted to expand on it a bit as having just one sheild can be a bit limiting, I haven’t been doing it long and would like to try some more advanced stuff. I will give this a try using more than one shield at a time until I can get the hang of it then possibly move on to doing it through breadboards. I find once you have an understanding of how it all links together, Makes it a lot easier to do it on your own. Thanks your have been a massive help!
Isn’t that just an FPGA?
Thanks, I knew there had to be something out their already invented for that, I am pretty new to E/E so still learning better when you know the name of the thing your looking for.
This was was off topic but probably because the article was meeeeehhhhhhhh.
Assuming you mean more than simple external 3-D imaging: Interesting idea, though as you mention it’s not yet practical to image the entire body for an entire population as CT is too hazardous, MRI too expensive and Ultrasound won’t do the job. One of the predicaments will be what to do about abnormalities, the true/false positives. Consider the case where images are not examined until many years later and upon inspection, a cancerous mass that would have been treated initially, has progressed beyond the point of treatment. Sounds like litigation time, regardless of any and all waivers signed beforehand. Consider the potentially many cases in which a mass is identified, leading to invasive/non-invasive treatment with increased morbidity.
I dont see how anyone would sue. As long as its made clear your just getting a scan, and no one is going to do any checking, they can hardly be blamed afterwards.
Who’s to say its even a medical person doing these scans at all?
Having been in the position of being sued after performing a procedure with at least 3, detailed and signed consent forms… people will sue for any reason and the cost (financial/emotional) is yours regardless. Additionally, you’re not “off the hook” simply by not being a “medical person”.
Perhaps you could go to a country where not every person is a full-blown raving lunatic to have the scan done, perhaps put the thing at airports.
CT and MRI are NOT the only imaging modalities. There are also (at least) PET and SPECT, which involve very little radiation. Nonetheless, medical imaging equipment is very expensive. I can go buy a car for $15k, yet one of these imaging machines, be it MRI, CAT, SPECT, or whatever, costs millions. Why? Is a car any less complicated? Plus a plain Jane car has to withstand a fairly hostile environment, while medical equipment—certainly the expensive imaging equipment—usually operates in a very controlled “office” environment. Why should an MRI machine cost 100× the price of a car? Time for hackers to change this!
Because they use pounds of rare earth metals in high purity, frequently make use of superconductivity which is expensive to maintain, precise motor control, sensitive and precise sensors, and licensed software to record and collate the data into something a human will recognize.
I’m not sure citing imaging techniques that use radioactive tracers as ‘little radiation’ is entirely accurate. A few pubmed articles state that a PET scan* is somewhere in between a dental x-ray and background radiation. Which doesn’t sound so bad, except that these tracers are designed to operate within your internal organs.
So 5-20 uS/MBq isn’t terribly high, but I wouldn’t design my company around giving people PET scans a few times a year so their jeans fit better.
*Depends entirely on the tracer used, but there is a minimum under which you cannot image. This is due to absorption by the body as well as sensor sensitivity.
It seems to me (not a doctor!) that setting a broken bone is not something that can be done progressively – that is, it must be set into the orientation desired for healing all at once, so that the body can heal the break. The alternative approach – moving the broken bone progressively over time – would mean that the body begins to heal the break *in an incorrect position* and that making each progressive move would require *breaking the partially-healed bone again.*
This is actually something that happens from time to time, though it is less common these days: broken bones which were set incorrectly must be re-broken in order to set them again correctly so that healing can begin anew. This is a painful prospect for the patient, and is regarded as a procedure to be avoided by setting the bone correctly the very first time.
For this reason, the Invisalign analogy breaks down: braces, including Invisalign, move healthy teeth progressively inside of nominally-healthy soft-tissue gums and healthy unbroken jawbone. Gums (soft tissue) adjust to compensate for the forces that braces apply to the teeth, and bone sockets compensate over months to harden appropriately beneath the gums.
In short, there are plenty of good therapeutic reasons to have high-resolution 3D scans as part of our medical records, but progressive bonesetting is probably not the best example.
This is very true.
Long ago I worked one on of the early dental crown scanner / CNC systems. The workflow involved making and digitizing impressions, then milling a new surface out of ceramic. The molds and scan data were kept briefly in case a replacement needed to be made. But for the exact reasons you mentioned there was no value in preserving the scans.
I remember reading about a technique which was pioneered in the USSR to treat injured WW2 soldiers whose legs ended up unequal lengths. portions of the leg bones were cut through leaving the marrow and soft tissue as intact as possible. An adjustable brace was placed on the limb which allowed it to be slowly stretched to the desired length. The marrow and soft tissue would stretch and over a period of time bone would fill in the gap.
Also works for when you are Ethan Hawk trying to pass as Jude Law.
GATTACA!!!
It was used in the USA up til at least the early 90s (the last time I was offered it) and probably is still used. Leg’s being apparently unequal length due scoliosis tilting my hip bone an inch and a half, they offered to stretch the “short” leg once I finished growing.
The brace, by that point in time, looked something like a halo device for stabilizing the neck after neck/spine surgery. It was screwed into the bone above and below a surgical break, and simultaneously stabilized and provided a method to stretch and re-break the limb every few days. Basically, re-breaking the bone every 2 or 3 days, moving it a few millimeters at a time, until it reached the ideal length; then allowing the bone to set completely.
Needless to say, I turned them down and admitted that I’d prefer a lift on my shoe to going through a month or more of this just so I could put on rented skates or ski boots again.
This only works if the growth plates haven’t fused. That is, before puberty is finished 17-22 for most males/females.
It works even afterward. The stretching isn’t occurring at the growth plate, it is happening at a surgical break in the bone. By opening up the leg/arm/whatever and sawing the middle of the bone to make two halfs, normally it would heal like normal. Instead, this rig stretches and re-breaks the bone every so often and causes the healing mechanism to make the bone longer.
3D Body scans, Organic 3D printing. Clones.
Anyone ever play Paranoia? That is what our world is heading. =) Clone Vats, broken Computers and insane laws.
But in all seriousness, 3D scanning of body parts would be useful if you lost a part and we had the tech to rebuild the parts people need. Oh, you lost your left leg? No problem, printing one out for you now.
3D scanned and 3D printed sex toys could be a market.
They already exist. Cynthia Plaster Caster was doing a similar things decades ago.
Add a Dilduino board with some motors and you have a vibrator =)
The one question I’d have is how often would you have to do it… it’s not like you scan yourself once and call it good… If your 12 and then grow up to be 21 and burn off a finger or two in a freak electronics accident, that 12 year old’s finger isn’t going to work too well.
Failing that… does anybody know of a good inexpensive 3d scanner for small parts. Small parts meaning something about the size of an HO model locomotive (about the size of a stapler)?
I see some, but they are thousands of dollars… they have to be getting cheaper by now.
I like the photoshopped screenshot from what looks a lot like the Futurama Space Pilot 3000 episode. It’s probably an open source image (no attribution required) right?
On a far more simple/cheap scale…would it be possible to make a crude “weight map” ?
That is, some sort of mat that tracks the weight distribution of the body. Lie on it each day at the same time (in the same position) and thus see not only your weight change over time, but also its arrangement.
Obviously there would be a lot of “noise” and I assume a low resolution. But Id be curious if some health issues couldn’t be picked up like that.
MRI’s are too expensive. CT scans expose you to too much radiation- max would be maybe 3 or for a year. Any more than 7 or 8 would increase your rate of cancer.
There is a technique for cheapish noninvasive imaging: sonography. It would be possible to build a sonograph into a bathtub, and use computer learning and frequent scans to detect rapid growths to identify and model structures.
Sonograms can’t detect leukemia, bone cancers, or anything in the brain or spine, and are very poor around the lungs. They can’t image through bone or air, and they cost as much as a new mustang, but I personally think its the best plan we’ve got for fighting cancers.
Are you talking about making the whole bathtub inner surface into a piezoelectric probe? I assume what you mean you can buy for the price of a “new mustang” is just a conventional ultrasound machine with its little probe, only able to see a funnel-shaped area right in front of it, with resolution falling off rapidly with distance? The probe manufacturing is quite complex. I used to work at an ultrasound company in the mid 90’s (but doing software, so I only saw the probe assembly area once). They started with whole crystals, sliced them into some kind of little rods or slivers, arranged those into a linear array, and each one needed its own micro-coax cable, bundled together into a cable with an enormous connector, so that it was possible for the electronics to send and receive signals from each one. All for just a linear sensor, like a linear CCD. 2D probes were considered out of reach due to the sheer scale of the electronics and cabling necessary. (And wikipedia still says now that 2D scanning is done by sweeping the beam.) So what I can imagine is that the electronics could be manufactured on a large silicon wafer or sheet, and then somehow piezo material could be deposited on top. The analog electronics would have to be right next to the crystal to avoid all that cabling. But AFAIK nobody has done that, and is there even a process for epitaxial deposition of piezoelectric crystal? A quick google search and I see that there is recent research on it, so I guess it’s at that stage, not ready for a real manufacturing process yet.
The bathtub had better be form-fitting so that the ultrasound doesn’t need to travel very far.
Became interested in 3D printing initially for only one purpose- print teeth on demand.
I have messed up teeth, and I always hated the idea that all they can do is get worse.
I can never exercise them and make them better. All they can do is decay, or halt decay.
I know teeth need to not be solid, they need to squish just a tiny bit, and no substance
yet known replicates the true durabilty of natural enamel and tooth structure.
I played around with the idea of getting 3D printed metal implants, ala Jaws,
but realized teeth fall out as you age due to bone loss. Human mouthes are not static
environments, dimensionally speaking, for something like a permanent insert.
Thought about doing porus material- like aerated titanium- for the jawline portion,
to slowly let the jawbone grow into and mesh the teeth more permanently, but realized
I’d be screwed if one broke- it’d be impossible to replace, and might snap my jaw or skull
with it.
Can 3D printed teeth truly be done? I refuse to simply live with only worsening teeth at
worst, already cavity ridden and staying that way forever at best!
Yes, if you’re talking about crowns for implants. There are a few ways: fusing powdered ceramic in a lost-material casting of a 3D printed positive (SLA resin, FDM plastic, or SLS wax), CNC milling from ceramic, and CNC or 3D printed SLS metal finished with porcelain. It’s been a while since I’ve been involved in this stuff so I don’t know what the state-of-the-art is.
But there’s not likely to be an alternative that uses grown bone or bone-analog. Titanium is a tried and true way to permanently attach something to bone and is used in many other fields besides dentistry.
As a medical doctor this piece had me wailing “Noooo!” from the first paragraph. Docs often joke about the futility in getting what we call a “pan-scan” when we’re concerned something’s up but can’t find anything using targeted testing. The biggest issue is the problem of incidental findings. Let’s say the lining of the thoracic cavity is a little thickened in one patch. Is that real and a potential early cancer or an artifact of the way the scan data is interpolated? When you’re doing a scan in a patient with pre-selected risk factors and assessing for a condition, then it’s most likely real. For example, if someone has been exposed to asbestos which can lead to a cancer along the pleural lining of the thorax (called mesothelioma) and you get a CT on them that shows thickening, than the odds of the thickening being real are high and you act on it. But if you take Joe Schmoe off the street who doesn’t have risk factors and see the thickening you have no idea what the odds are that the thickening is real. You then have to decide, do I jab a needle into the chest to get a piece of that lining to look for cancer and risk dropping a lung, bleeding or infection? If the sample is negative is it because there’s truly no cancer or did I miss the spot with the needle? Do I instead get a repeat scan in 6 months and risk losing time and exposing the patient to more radiation and 6 months of stress?
Mike’s proposed solution is to not interpret the results unless they’re needed down the line. Well now you’ve spent a LOT of money for nothing. Also if using CT scanners you’ve exposed people to radiation, with a risk of 20 cancers per 10,000 total body scans done in 30 year olds. (http://www.ncbi.nlm.nih.gov/pubmed/20008689) If using MRI scanners people are exposed to not-insignificant claustrophobia and LOTS and LOTS of cost. All this for the possibility that sometime in the future there might potentially be a benefit of unknown magnitude? Sounds like the suckers who pay to get their heads frozen after they die.
Patrick, we have no way of confirming your a “real” board certified doctor. But your post if welcome. I wish more people/patients understood that you’re not paying a doctor to do/research something you can do at home on the internet. You’re paying a doctor for his clinical “actual” experience. His/her ability to have seen the problem, even thought the symptoms do nothing more than make the problem hard to see. People forget that.
I agree. This is similar to the hype over IoT in that there’s no value in collecting as much data as possible if you don’t know what to do with it.
My dad died from a very rare disease that, in retrospect, could have been diagnosed a year earlier when treatment would have been effective. But none of the doctors who made the early observations knew enough about the disease to request follow-up testing that would have led to a diagnosis. The doctors were exceptionally competent in their areas, but even if they knew about the disease they would have still dismissed it as unlikely.
He had quite a few x-rays, CT scans, MRIs, and every blood panel known to man, but the volume of data was not enough to guide the doctors in the right direction. The first observations, which were very much qualitative and made during a seemingly unrelated procedure, remained the best clues for quite a while. Perhaps in the future this could be solved through “big data” correlation of similar cases, but with the current methods for diagnosis it’s impossible to avoid these outliers.
“Perhaps in the future this could be solved through “big data” correlation of similar cases, but with the current methods for diagnosis it’s impossible to avoid these outliers.”
How would big data ever learn to correlate without the dataset to train it though?
“The biggest issue is the problem of incidental findings. Let’s say the lining of the thoracic cavity is a little thickened in one patch. Is that real and a potential early cancer or an artifact of the way the scan data is interpolated?”
Isn’t it wrong to blame the data for that though?
In other areas of science I don’t think we generally say “theres too much data” when there is “noise” and “false positives”. Rather attempts are made to pin-down and isolate the differences. Identify what patterns we can.
For sure the general population cant do this, and over diagnose is a problem. But I think its wrong to infer thats because theres too much data. Perhaps if more people were exposed to “normal variance” and “unpredictability” in what their insides can look like and the various ways it can be interpreted they would be less willing to jump to conclusions?
Of course, cost and safety are legitimate issues here.
Merely talking about hypothetical “magic” free scans or whatever.
> For example, if someone has been exposed to asbestos which can lead to a cancer along the pleural lining of the thorax (called mesothelioma) and you get a CT on them that shows thickening, than the odds of the thickening being real are high and you act on it. But if you take Joe Schmoe off the street who doesn’t have risk factors and see the thickening you have no idea what the odds are that the thickening is real.
I understand your point, and your concern. But like other commenters have pointed out, more data won’t make you more wrong about a diagnosis (if you’re using it correctly to update your priors, see Baysian Statistics https://en.wikipedia.org/wiki/Bayes'_theorem).
Your concern would be that we see a thickening in someone without the other risk factors (asbestos exposure), and treat them the same as someone with the other risk factors. This would just be bad statistics (and I understand how this can and would happen in the real world, and that *is* a concern, but not one that couldn’t be treated with training and digital tools). For years, doctors have only done the scan on people with other risk factors, so by the point they see a scan, if they see thickening, the next step is intervention. But a good Baysian knows that the order in which you receive your evidence doesn’t matter; whether the scan happens first, or I ask about risk factors first, the evidence is the same, and I can choose to act on it in the same way I always have.
But now I also have the option to act on it in new ways. Before, I would have had no information about how prevalent thickening was in the general (no risk factors) population. That’s useful information that will help me eliminate both unnecessary surgeries, and missing surgeries that should have happened.
Scans are good for people, as long as the process gets updated to handle the new information in the correct way.
I get an MRI every few years, CAT scans when needed, radioactive isotope scans every 2 years or so, and for 20 years got X-rays every 6 months to a year. Mostly focused on my spine, but not always.
Over a period of just 6 months, the X-rays would change dramatically. Which foot was my weight balanced more on? Did I have shoes on or not? Holding a very deep breath, or had I exhaled and held that?
The CAT and MRI I’ve learned to render in POV-Ray so I can rotate things in 3D and see what a trained radiologist learns to interpret, and from that learned to read some-what well (to the point that I found a defect that the radiologist missed). What is it worth 6 months later? Not a whole lot. “But Quin,” I hear someone yell, “Mike has his teeth molded in case of an accident!” and that’s great. Your teeth don’t move a whole lot once you hit adulthood. “Your other bones don’t grow either!” I hear. And true, they don’t. But short of decimating trauma, in which case you should be happy they can put you back together at all, a 6 month old scan would only be useful in putting things back in roughly the same place. Why? Because even if your teeth get knocked out they can only put back the ones that you find. In a compound fracture, some of that exposed bone is going to die and if you force everything back “exactly” like it was before you may end up with a longer healing time or worse.
But a one year old full body MRI scan, with the broad target of “every organ and bone” is going to be pretty vague in detail for any of those specific organs or bones. Those things require a good bit of focusing, with the result being something like macro-photography with focus-stacking. If you got all the fore-ground and background details in a macro photo, you wouldn’t feel the real depth involved. Same thing applies. My spine specific MRIs from a few years ago aren’t useful to a doctor now because my condition can result in bone structure changes and degeneration, and spines have those funny pieces of cartilage that can change really quickly.
My opinion as someone who gets those scans pretty often is that the use for the general populace would be very limited. The chance that you got the right scan with the right target recently enough to be useful is slight; and any emergency, or even new symptom, is going to get you sent for new scans to make sure that whatever-it-is isn’t alone.
I’m pretty sure we need something more practical first – like shoe technology. Wouldn’t it be amazing if there were scanners in shoe stores that could 3D image your feet so you get the perfect shoe fit every time? We could make them really cheap too and use X-Ray emitters and skip any shielding for pregnant mom’s standing nearby with future 3 armed siblings.
There are a few warning signs on the technological super-highway.
And what about the airport scanners? Can’t we just use them, ask if we can keep the 3d images ?
Didn’t the US stop with the back-scatter (RNA-activating health risk) devices?