
Bryan is a computer neophyte (he needs help turning his computer on), but he has a basketball story. His team was playing in a crucial basketball playoff game at the club. They were down by two late in the game and he just couldn’t get one of his players to play defense. This player was a great shooter and that is about it — burying a three that put the team up for the first time. After sinking it he just stood there admiring his masterpiece while Bryan screamed at him to get back on defense (he rarely played D and he didn’t that game either). Instead, he flat lined and went down on his face– heart attack!
Of course that player was me and that was an awful day. But I’m still around to tell the story… as a hardware designer years before I didn’t know that I’d bet everything on one particular project.
Simple Beginnings

My name is Chris. In the seventies, I got a degree in EE from MSU (the good Michigan University!). I also took some bioengineering and computer programming classes. In the back of my mind, I thought I could cure my diabetes with some kind of technology. I could type punch cards with the best of them. I am pretty sure that the beer I consumed was recommended medicine for using the CDC 6500 (well, except when the cards fell on the floor before I could give them to the operators. I chose to blame them).
When I graduated, I went to work for a large airplane company. One of the jobs was as an automated test engineer. I created circuit boards and software to test all of the electronics on a plane before it could fly. The (mighty) HP1000/RTE, programming with Fortan77, Macro/1000, SymbolicDebug/1000, and machine languages to talk to the chips. My beer drinking friends would always get nervous when I would tell them that the plane wouldn’t go until my tests gave it the OK.
I soon abandoned the big company bureaucracy. I went to work at a local hospital. Working on an ECG (Electrocardiography) analysis computer. The system used artificial intelligence and pattern recognition software and knowledge bases to automatically carry out the interpretation, test reporting, and computer-aided diagnosis of ECG tracings obtained from a patient. I used the (mighty) HP1000/RTE again, with 4 platter removable disk drives that could hold about 300MB of data and tape backups.
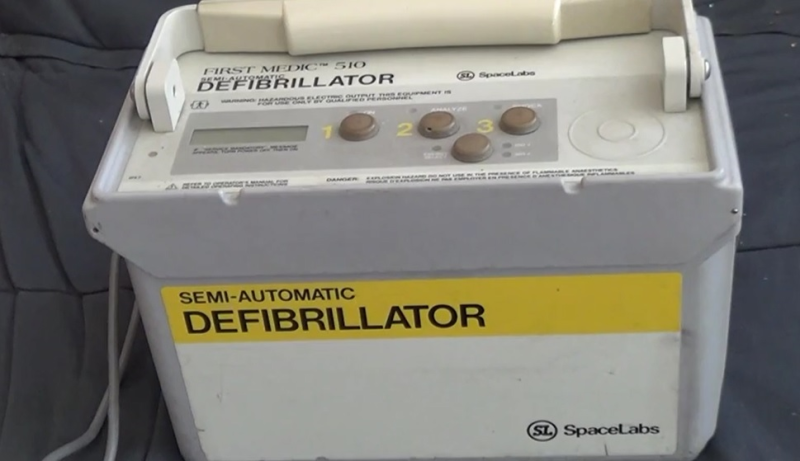
The cardiologist I worked for invested in a small startup that was going to make semi-automatic defibrillators that could be taken out into the field by first responders (police and fire). With heart attacks, the quicker you get the heart back, the better chances for survival. At the time, only EMTs and trained specialists could bring out the trusty paddles and administer a shock. But that might take precious time to get them to the scene.
To develop their defibrillator algorithms the company, First Medic, wanted to use the years of ECG data my system had gathered. I was their first consultant. It was fun and exciting (plus, they had also hired a friend of mine who worked at the plane company), so I only charged them a case of Sam Adam’s beer for my work (hey, it was good beer!).
I went to work for the company a short time later. The defibrillator had to be small and portable, pack a punch (up to 360J of energy per shock), have rechargeable batteries (which was hard back then), not fry the chips with the high energy shocks, talk to the operator to tell them what to do next, read the patient’s ECG and decide when to shock. Then, after the incident, the system had to communicate results with hospitals, and have a data management system. We built small cartridges to plug into the machines. I built a device that would read that data and transmit to a computer via a serial port or over a modem. I did the data management system and all of the communications software. Had to do it all on DOS machines with 640K max, as fire and police had limited budgets for another computer system that only ran this system. I created printer drivers for dot matrix printers and later laser jet printers. I had to create graphics to view the ECG on the computer … and graphics were a bitch on DOS machines! I used C, Assembly and various machine languages to program.
Like many startups, we invented new technology, the work was interesting/challenging/fun, and we ‘changed the world’. However, we ran into regulations, as we had to go from state to state to get them to change the laws to allow non-doctor first responders to deliver shocks. You may be surprised to hear that it probably took more time and resources than actually building the product. To make matters worse, we had foreign investors who bailed. We ran out of money and got purchased by another company (for pennies on the dollar) before finally releasing the initial product. How often does the first one out of the box not make the big payday? We would ask for pay and get more stock options. I wish I had kept them, as I need the wallpaper.
Back to the hoop story


Two teenagers sprinted out onto the court and gave me CPR. But, more important, grabbed the easy-to-use AED (which the club had just bought and trained its employees to use) and re-started my heart. Two weeks later, I was released from the hospital. Two intrepid teenagers and a brand new AED had saved my life.
Bryan is glad I was saved so that I can go over to his house to turn his computer on!
Learn more about the First Medic 510 Automatic External Defibrillator from this demonstration video or the original spec sheet (PDF).
About the Author
Chris, more than eight years after his death defying act, is working at the University of Washington. He is building out data systems for multi-center biomedical research studies in an effort to improve people’s health and lives.













I have “saves” using early AEDs while on rescue calls. We were the second Squad in Burlington County NJ to get a save with an AED back in the early 90’s, Marlton township beat us by a week. We didn’t care, we were a tad ecstatic that we could start revitalization before ALS arrived.
That must have felt great to actually be able to do something about it rather than just wait and hope.
Reblogged this on The Cryptosphere and commented:
A great first-person tale of how hardware engineering saves lives every day. Thousands of people who otherwise would have died have instead been saved by these devices, now common in public facilities like schools and arenas. One very real way that miniaturization has effected the world; previous models were too bulky to store, too complex for “civilians” to use.
Dag dude, This one brought tears to my eyes.
That was a great story, I’m glad you are here to share it.
This type of stuff is why I like working in healthcare IT. People ask what’s so enjoyable — I tell them it’s saving lives through SQL statements! And JavaScript. And HL7. Technology!
Thanks for that. I almost fell from my chair and broke my neck (no amount of SQL would fix it) . I also work in healthcare IT and i thing there is more focus on statistics and proper it security than the patients. And IT allows for more bureaucracy than ever. Instead of streamlining the process for MD’s and technicians like i used to i find myself adjusting to ever changing reporting fiscal analysis and proper codes and markings for our government health insurer.
Healthcare IT and security? LOL, nice one… (maybe that magical place exists. if it does, I haven’t been there yet, all healthcare IT systems I’ve worked on/been otherwise exposed to were HORRIBLE)
Now that the Federal Government is handling healthcare, the healthcare providers no longer have to worry about having terrible HIPPA security, I’m sure the government’s security will be far worse! B^)
The federal government isn’t handling healthcare. At least, no more than it has in the past.
Do you live in an alternate reality where the USA got a single-payer option? I’d like to live there, too.
Yeah that’s why i’m working on it a lot … once the online data sharing will start in 2017 all hell will break loose. And my system is fairly secure … so what … MDs are sending patient data via unencrypted email ….
Man, I feel sorry for you with the new ICD update
Wow. Just wow.
I wonder how much of your work is now built into the defibrillator that’s implanted in my chest. If any, even a small sliver of your work, or if you influenced in any way the people who designed and built it, then I have to say a great big Thank You! It’s had to shock me twice now, and I’m glad it’s there. So, Thank You, a million times over, for saving MY life!
(sniff!)
My brother-in-law was saved by an AED only a few months ago. Thanks for the story, and thanks for working on lifesaving technology.
Heartwarming… for the serendipitous save of someone by a device they (helped) create, but also for memories of the HP1000 and RTE IVB (tugging on my grey beard). Not to detract from the otherwise great story, but “flat line” (also called asystole) is not generally a shockable rhythm despite what is seen on popular media.
Darwin 0 Technology 1
the things we can now do with medicine etc depend on what darwin and others discovered about our origins. this is a win for darwin just as much as a win for the technology we now have as a result of not thinking we came from mud or some guys rib.
Darwin (temporary) 0 Technology (temporary) 1. Darwin always wins in the end, unless we find ways to reverse engineer and simulate/rebuild the brain in silicon and thereby make an immortal mind.
You don’t need to be immortal to win at Darwin’s game; just have fertile offspring.
This! I bet that the reason his portraits look so grandfatherly…..
fantastic post! wow. just wow.
I’ve been in tactical and emergency medicine for almost 25 years, and happily using your products (or the descendants) for most of that time. I’ve hacked many of my EKG systems for years (The 12-Lead MAC’s use essentially the same software as when I first learned to use them), and always wondered about the rhythm interpretation software. We used to tell students “The software is frequently wrong” and then tell our residents/graduates “The software is fantastic. If you don’t agree with the interpretation, make damn sure you’re right”. The software is fantastic, and a smart person will use it as a second opinion on their cardiac cases.
I can’t tell you how many times I’ve put leads and patches on people, using your software. Hell, in the field, there are a bunch of cases where we just can’t read the EKG to do a real interpretation (the screen is too small, not enough resolution, no paper, etc. You go to battle with the gear you got). In a crunch, we’re using your work to treat. You’re saving lives, and will continue to do so long after you’re gone.
Huge thanks, and I’m glad you were in a position to benefit from your work!
(Sorry you wound up there, but glad your gear was on hand. You know what I mean…)
Not that I’m a doctor or anything, but an AED “stops” your heart from fibrillating. It doesn’t “start” it
One could consider a fibrillating heart to have stopped in the sense that it is no longer functioning and that stopping it is restarting the hearts normal operation.
This makes me feel even better about having an AED at our hackerspace. None of us are cardiologists so I don’t think we’ll be diving into its diagnostic interfaces any time soon, but it’s really cool to read the inside story of how these things came to be.
I hope we never need it, but I’ll thank you that it exists, in case we ever do.
Great story. You jumpstarted the technology and it returned the favor.
If you want to see inside a couple of AEDs, I did some teardowns a while ago :
http://www.youtube.com/watch?v=pn-Wv9YAfv0
http://www.youtube.com/watch?v=eWC22NufDUo
And an implantable one :
http://www.youtube.com/watch?v=Gzw6c3Bi4TU
I remember that first video! I watched it twice, learnt a whole lot man. Thank you
Really like the tear down videos and all of your work in general Mike.
Thanks for sharing.
really touching
An amazing story!
THIS is why I love working in this industry. I work on this kind of equipment every day, all year round, and while I know on an intellectual level what it’s capable of I have to admit this is one awesome story, to not only hear about the early development of the Automated defibrillator but to have it save your life in the future…. . . . I don’t even know how to describe how cool that is to me!
@Rocky Essing : You are partially correct, any defibrillator will stop a heart that is ‘fibrillating’, which is the rapid, erratic unsynchronized contraction of the muscle fibers. What people often are referring to when a defibrillator ‘restarts’ your heart is it helps restore the normal contraction of the muscle fibers associated with a good heartbeat.
Something to keep in mind is that AED’s are not effective for all heart attacks, right now they are only capable of defibrillating Ventricular tachycardia (Vtach) and Ventricular fibrillation (Vfib). This is because the AED needs some kind of heartbeat or contraction to restore, they are unable to restart a ‘flatlined’ heart (no heartbeat at all , i.e. asystole) Still, the fact that many of these devices can work ‘hands off’ and fully automatic. or even semiautomatic of when to shock is an amazing technology for the non-paramedic to be able to use to save a life.
Yes, it’s best to have some training, but most of them are as simple as this
1) open the package and apply the pads per the diagram *remove metal objects such as underwire bra’s if patient is wearing one*
2) turn unit on and do not touch patient
then if a semiautomated AED
3)press the ‘shock’ button when told
If it’s the fully automatic model, you don’t even need to do step 3. It’s that simple. Part of my job is to test the operation of the defibrillators in the hospital with a defibrillator tester, which can simulate various heartbeats. For the above noted irregular heartbeats, they work just hat simple.
Now I’m hearing that old Jeff Goldblum iMac commercial. “There’s no step three. There’s no step three!” ;-)
(Bollocks on that! I did ISP tech support and getting a Mac online had at least as many steps as Windows.)
My favorite time was when I was reading this on HaD.. then tabbed over to my feeds.. and read it again on /. , WTG Szczys!
You rock Chris.
I was working at a small medical device company in the early nineties developing a fiber-optic pressure transducer for monitoring intra-cranial pressure of head trauma patients. We had sent out units for clinical trials. I was watching the evening news after the Oklahoma City bombing and the news footage showed one of the rescued children in the ICU. Sitting next to her was the electronics unit I had developed with a transducer attached. That 10 seconds of footage made all my hard work worthwile.
In 2006, we have started a project of an open source hardware/software defibrillator. A spanish foundation was interested by funding the project, and had to make a collective decision to fund or not. But the project was rejected by some people in the jury involved in the business of medical aid… at this time our calculation was to produce a defibrillator for around 300$ ( instead of 1000 or more for industrial ones).
I have always felt that Karma was somehow real. This account only reinforces that feeling. Great that Chris is still around to developed more awesome stuff, no pressure to perform implied Chris, this is many more times that most off us will be able to contribute.
I’m really happy my brother saved his own life. We have become friends as siblings and I respect and cherish our relationship. I would be sad if he had died. And it’s pretty cool to save yourself with technology!
Besides all the other great comments on how cool the story is, etc. I’d like to say that Chris not only was very talented but he had a marvelous job where he got to innovate and create at multiple levels and disciplines. That sounds very appealing. He sounded like a jack of all trades, master of all to me.
Have to say an amazing story and cant imagine how many times the code has been used. Only comment I would make is the basic mistake of saying Heart Attack, you do not use a defibrillator on a casualty having a Heart Attack, you use them on Cardiac Arrest. Two different conditions, Heart Attack can lead to Cardiac Arrest but not treated the same. Otherwise, well done, fantastic story.
Great story! The ripple effect comes to mind here.
This is just great Chris. Funny, moving and important. Thank you.
Great story, well told! I’m glad you were there for you! :-)
This is great, and Chris, glad to hear it worked. You may remember that I was the emergency physician that was part of 1st medic. From many years of experience I can tell you we have saved thousands of lives with this tecnology. I am still working as an ambulance service medical director and our first responders save lives every month.
Great story. I am so glad you survived your cardiac arrest. Small world. I was a statistician and programmer who worked with a team at King County (WA) EMS in the 80s that was doing research with AEDs. We tested a device called the HeartAid from a company in Portland (just found a link to it here… http://www.emsmuseum.org/virtual-museum/equipment/articles/402161-Cardiac-Resuscitation-HeartAid) and later moved on to work with Physio Control, and other devices. It was an exciting time but it was so cool later on to see the widespread deployment of AEDs everywhere including the floor of my building at Fred Hutchinson Cancer Research Center. And I’ve been trained to use it too.
Oh Chris – Saving lives 1 beer / 1 bit at a time
So awesome to know you