Did you get a flu shot this year? How about last year? In a world of next-day delivery and instant downloads, making the yearly pilgrimage to the doctor or the minute clinic feels like an outdated concept. Even if you get your shots free at the office, it’s still a pain to have to get vaccinated every year.
Unfortunately, there’s really no other way to deal with the annual threat of influenza. There’s no single vaccine for the flu because there are multiple strains that are always mutating. Unlike other viruses with one-and-done vaccinations, influenza is a moving target. Developing, producing, and distributing millions of vaccines every year is a massive operation that never stops, or even slows down a little bit. It’s basically Santa Claus territory — if Santa Claus delivered us all from mass epidemics.
The numbers are staggering. For the 2018-19 season, as in last year, there were 169.1 million doses distributed in the United States, up from 155.3 million doses the year before. How do they do it? We’re gonna roll up our sleeves and take a stab at it.

A Shot in the Dark
Although humans have endured seasonal misery for thousands of years, the first influenza virus was not identified until the 1930s. Before that, everyone thought influenza was caused by a strain of bacteria. The first influenza vaccine was created by Jonas Salk and Thomas Francis. Salk would use what he learned to eventually develop the polio vaccine in the early 1950s.
This beta-level flu shot protected against only one strain of influenza A. It was first used on soldiers in WWII before becoming available to the public. Since then, flu vaccines have evolved to target multiple strains of types A and B. These days, manufacturers are producing both trivalent vaccines, which cover two strains of influenza A and one strain of B, and quadrivalent vaccines that cover two strains of A and two strains of B.

A Race That Never Ends
Producing the modern flu vaccine is a year-round effort. As the flu season comes to an end in late February or early March, the World Health Organization, CDC, NIH, and FDA get together and develop a plan to tackle the upcoming season. They look at the strains from the season that just ended, and they look at what’s beginning to circulate in the southern hemisphere. From there, they try to predict what strains will show up in the coming fall.
Then they make recommendations to the private manufacturers who produce the vaccines about the strains they should cover. They also send candidate vaccine viruses to the manufacturers — seed viruses grown in chicken eggs — to get them started.
Finally, the manufacturers get to work creating their vaccines. They only have a few months to develop, test, and submit sample vaccines and test results to the FDA. Then the FDA does their own testing, and by late summer will begin to release lots back to the manufacturers. As soon as they are deemed okay, the manufacturers start shipping the shots.

You Gotta Break a Few Million Eggs
The oldest method for developing influenza vaccines involves fertilized chicken eggs. Each egg is tested to make sure it contains a viable embryo and is free from infection. The good eggs are washed, injected with flu virus, and left to incubate and multiply the viruses for four or five days. Then the viruses are extracted from the eggs, killed with heat, and loaded into syringes and vials.
Not everyone is tolerant of eggs or needles. Completely egg-free vaccines are produced using recombinant technology. The recombinant process isolates the hemagglutinin (HA) influenza virus gene and reproduces it inside insect cells with the help of another virus that excels at growing inside insect cells. When it’s time to package the vaccine, the HA protein is harvested from the cells and purified before packaging.
There is a third process known as the cell-based vaccine. In this method, viruses are grown inside of cultured cells from various mammals. Interestingly, this process was approved by the FDA for use starting in 2012, just one year before the recombinant process was approved. Up until the 2019-2020 flu season, cell-based vaccines were always the end result of cultures that originated as egg-grown vaccines. But this year marks the first completely egg-free, cell-based vaccine.
For the needle-shy, there is also a nasal mist version. This type of vaccine contains live but weakened flu virus strains, whereas the strains in the injected versions are completely inactive.
Walking on Eggshells
This annual race isn’t always a smooth run. One year there was an egg shortage because of avian flu. It’s no surprise that our vaccine production system is so dependent on eggs since there is a huge supply chain already in place. But the egg supply is always vulnerable to disruptions like the avian flu, and that’s one reason makers are trying to get away from egg-based manufacturing and move toward recombinant and other methods.
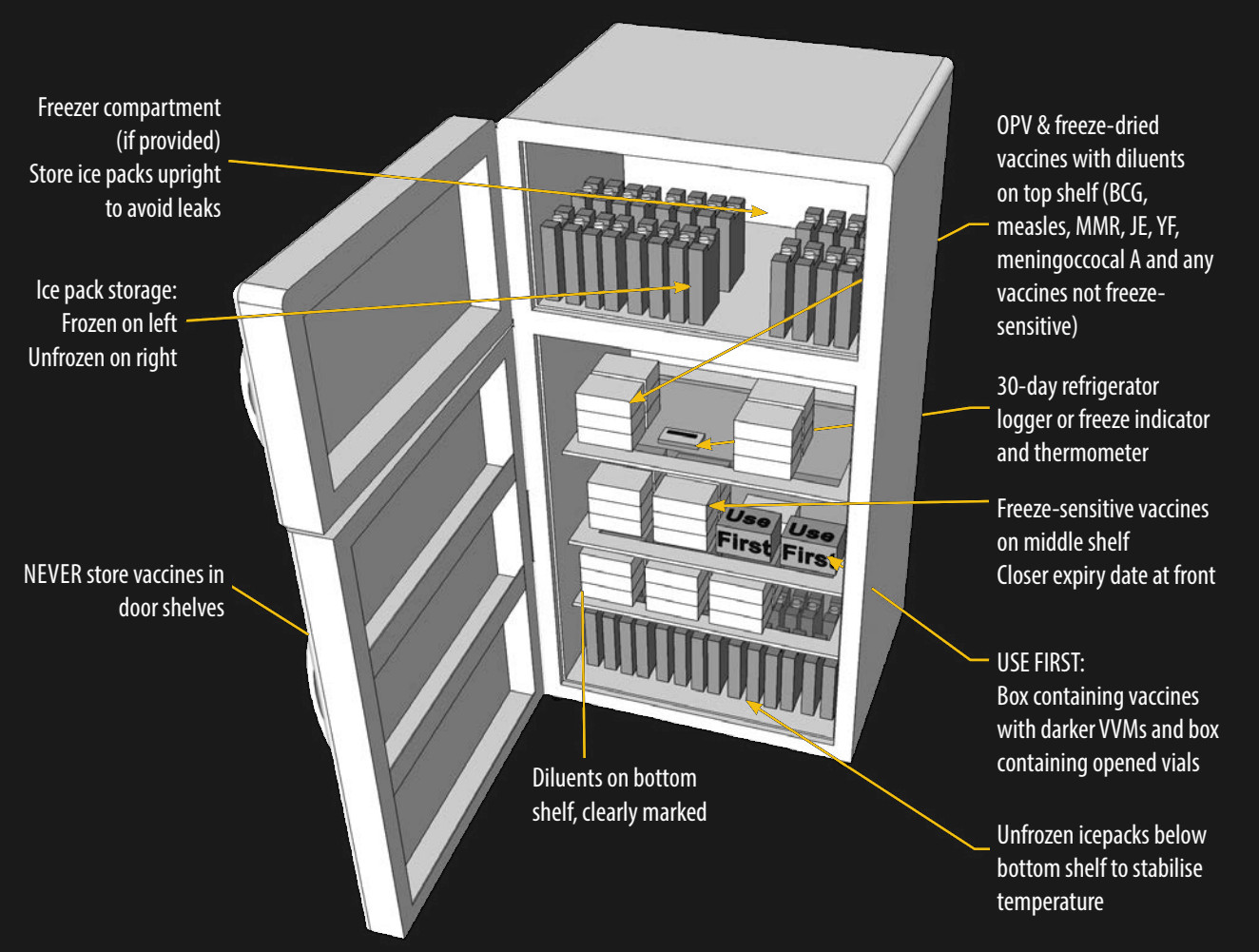
Logistically speaking, the vaccines require cold transport every step of the way, because influenza vaccines are quite susceptible to heat. You may find it of interest that there’s a whole cold chain required by the CDC (PDF) to keep the vaccines cold enough, but not frozen. It covers things like what type of cold storage devices to use, the location inside of those appliances that should be used for storage, and the type of hardware to use for temperature monitoring.
No matter how you take your vaccine, there is hope for a more infrequent dosing schedule. Researchers recently identified three new antibodies that bind to a different influenza virus protein known as neuraminidase (NA). These NA proteins change less frequently than HA proteins, so developing a vaccine that triggers the human body to defend against NA proteins instead could mean equal protection with less frequent vaccinations. Hey, it’s worth a shot.













>vaccination
>against viruses
10/10 would laugh again.
I don’t get it.
obviously ridiculing antivaxxers isn’t one of your pastimes….probably a good thing all told.
Oh Martin…
Antibiotics, also known as antibacterials do fight bacteria. They don’t fight viruses.
A vaccine provides acquired immunity to a particular disease. This is a terminology thing, it doesn’t necessarily mean bacteria or virus, just that its intent is to make you immune.
Antibiotics do not work agains viruses. They do work agains bacteria.
I see. Nevermind. Do not feed the trolls.
I am not a medical expert by any means but I have a question.
“These NA proteins change less frequently than HA proteins, so developing a vaccine that triggers the human body to defend against NA proteins instead could mean equal protection with less frequent vaccinations”
This confuses me. I would expect that if NA changes less frequently then the vaccination is more likely to actually work. Since as discussed the vaccination is a sort of best guess based on the current state of the flu and how it appears to be changing, if we could target a section that changes less often wouldn’t we be more likely to create a working flu vaccine? Obviously it has the benefit you describe of requesting less frequent vaccination which logistically is of huge value but for the elderly and the young/sick wouldn’t the appeal be the greater likelihood of effective vaccination?
The question is, effective against *what*. The reason an NA-protein vaccine could “work longer” is because it would be viable defense against a greater range of influenza strains. An HA protein vaccine is still highly effective, but only against the limited number of strains it covers. When people get the flu despite having received the vaccine, it’s because they got a strain not covered by their vaccination.
This is exactly the point. More effective for a longer period => Less frequent vaccination needed.
Yes I agreed with the point I was simply saying I wasn’t sure that was the biggest appeal.
I thought the bigger appeal would be the increased likelihood the vaccine was effective against whatever strains are currently roaming around. For people I know who are dependent on herd immunity the biggest concern to their health is not how long until the next flu vaccine comes out but what are the odds the current one will keep people healthy.
I’m not understanding your confusion… You seem to be in vehement agreement.
Targeting NA means the vaccine is more likely to work and will be effective for longer before mutation of the circulating strain renders the vaccine ineffective (these two performance metrics are tightly coupled, perhaps this is your confusion?)
As an example of how stable NA is as a target – Tamiflu targets NA.
Interestingly, there are very few mutations that confer oseltamivir resistance, hinting strongly that there aren’t many NA variations for a vaccine to target. Also, for whatever reason, these mutations are pretty rare, hinting that they may confer a serious evolutionary disadvantage to the virus when oseltamivir is not present?
Hackaday—
If you don’t watch your step, you’re going to get a REALLY bad reputation for printing very good, authoritative articles. This, by Kristina Panos, is not only very well written, but extremely informative and educational, and–obviously–speaks from no small amount of authority.
Very well done, Ms. Panos.
Flu vaccinations make me ill (have always been sick for 48 to 72 hours after the vaccination); and four of the nine times that I have been vaccinated, flu was still contracted several weeks or several months later. No other types of inoculations/ vaccinations make me sick.
Is there a percentage of humans where these flu vaccines are never or seldom effective? Or perhaps, as the wife-unit has oft claimed, I am not human.
Yes, my comment is worthless and nothing other than anecdotal information. But this seems to be indicative of a problem in the life sciences where ‘best practices’ result in less reproducible outcomes compared to the stuff of electrical and mechanical engineering.
There is a very long lead time to producing the vaccines, so they have to make some guesses way ahead before the flu hits. If the actual flu is different than what the vaccine was designed for, then it won’t be effective.
You body likely thinks that it had been inflected, so it try to fight it off. Most of the symptoms are defense mechanisms e.g runny nose, high fever etc.
My own anecdotal: I had my flu shot and because of family emergency I had to travel to a city heavily affect by the flu that the hospitals are full. I had to visit family member daily in the hospital. Didn’t catch a flu. :P
:)
My anecdotal: 1-2 years ago, I caught flu for the first time in my life. It was a year where the vaccine was already documented as having “missed the mark” by a decent amount as far as predicting the strain. One of my coworkers’ families all had the flu (despite the shot) – apparently the one unvaccinated person DID get hit much harder.
I got sick the next week, but even though I started Tamiflu past the usual “48 hours after first symptoms” guideline, it was highly effective. I credit the vaccine for slowing down the infection enough to buy me extra time for a Tamiflu prescription.
That’s the challenge with “effectiveness” metrics – right now, flu shot effectiveness is basically binary for each person in the sampling – either you got the flu or you didn’t.
If the vaccine was partially effective (slowed your flu down, reduced severity), current effectiveness metrics assign those cases to the 0% pool.
In my experience sometimes the flu shot will have some side effects and sometimes it won’t. Usually I just get sore in the area of the injection the next day but sometimes I may get a minor fever and headaches for a day or two. My sister though reacts more like you described so she rarely gets vaxxed if she doesn’t absolutely have to. I have also had folks tell me that they always seem to get sick even with the shot yet others don’t even though they got dosed around the same time and had similar exposure to the public like working in the same office or shop and interacting with each other.
I am also curious about what can cause such differences in otherwise healthy people of similar circumstance. Maybe over the next few years we’ll see more answers for questions like this since there are initiatives like that All of us program here in the US to study how different factors effect health in the population in different ways.
Actually I get worried if I don’t get a bit of a hot spot where the vaccination was, like my immune system just went “meh, so what” and didn’t make any antibodies.
I’m in the “sore arm for three days” category.
I think once I did get a blip of a fever for one day.
Some mild flu-like symptoms after the vaccine are not uncommon, but the vaccine does work. 99% of the time, when people think they have the flu, it is just a cold. You probably just had colds, which the flu vaccine does not address. A real flu (as in influenza virus) is a lot more serious- as in, it has a decent chance of killing you. People conflate colds and flus, but they are very different things in terms of commonality and severity.
This!
If you have the actual Flu, you’ll know it.
I remember lying in bed, incredibly thirsty, looking at the glass of water next to me on the bed side table and not having the energy to get it.
After that, I get frustrated by people who take a day off work with sniffles and come back saying they had the flu.
I had flu for the first time last year. I was well aware that I’d only had colds before that, but I didn’t know just how bad flu is. I live alone and was thinking what would happen if I died in my bed.
At work, they occasionally send out notices that a “flu or severe cold” is going around.
d*mn it, TELL ME WHAT IT IS. Severe colds suck but aren’t a serious health hazard, flu is a major health hazard for me as a Type I diabetic.
I don’t understand where your number, 99%, comes from and you provide no citation. Looking at these data tables on Vaccine Effectiveness (VE) from the CDC, they’re no where close to 99% effective. I routinely see numbers like this published in articles and placed in comments, but they don’t seem to reflect the CDC’s own data on vaccines. Please provide a cite so that I can review the supporting data.
Quinn’s point wasn’t that the flu vaccine is 99% (or whatever) effective, but just that most people who aren’t doctors will say that they’ve got “the flu” when they don’t have influenza. It’s just a very common misuse of language.
The real deal is a week in bed + weeks of recovery until you’re back to full strength. Having had it twice in my life, I don’t want it again. And I certainly don’t mistake random winter illnesses for the flu!
But thanks for the numbers on the estimated effectiveness of the flu shot. 40%-60% is kinda unimpressive, in a way, certainly compared to other vaccines. Still, if the cost is a few bucks, a shot in the arm, and a chance of a mild cold-like reaction against a 50% decreased likelihood of getting a very crappy illness, I’ll take it. And the more people who get immunized, the lower the chance that we all get it — herd immunity and so on — so you’re also doing your part to keep the flu in check.
In case others missed the link: cdc.gov/flu/vaccines-work/2018-2019.html
There’s also the added bonus that if you still get the flu after having the shot its usually not quite as bad. I’ve had the flu three times in my life; the first in high school which led to me getting the yearly shots ever since, the second time a couple years ago when I missed getting the shot when it was first available, and the last time was two years ago.
Both times I didn’t get the shot it was a week in bed and another two weeks or so until I felt right again. The time I had the flu with the shot I still felt like crap for about a week but I wasn’t completely wiped out so could still get some stuff done and then recovered faster. Anecdotal evidence again but that was my experience at least.
I wish I could reply to Bigfoot of Borg’s comment directly but there is no reply option…
My experience is the same as his. I’ve gotten the flu once, and it was a year I’d had the shot. However, Tamiflu was highly effective for me despite being past the usual 48-hours-from-first-symptoms guidelines.
Admittedly anecdotal, but I think I would have fared much worse without the shot. A coworker’s family had one unvaccinated person and they got hit harder than the vaccinated family members.
Sometimes (very rare) there are non-responders to some vaccines. If you suspect this, you could go to a lab for an antibody-titer after the vaccination.
The negative reaction could also be of an allergic type, then another type of vaccine could help. I can not remember that I ever had negative vaccine-reactions. But that is also “only anecdotal”.
The vaccine is not fully effective for about 14 days. It does not cover all the strains. So yes, you could get the flu every year after a flu shot, but you did not get it from the shot itself. You are just very unlucky. Stay away from casinos and sky-diving.
Maybe changes in lifestyle will lower the rate of flu. Don’t they all come from the rural Southern China virus factories? Family/village farms where the baby’s poop is eaten by the dogs and the dog poop is eaten by the pigs and the pig poop is eaten by the ducks and the duck poop is eaten by the carp and the carp poop in the water the people drink? This multi-species incubator was the source of the Spanish Flu and Bird Flue and Swine Flu, etc. At least I think I read that somewhere.
Viruses mixing between species does happen, but it’s not the only way that new flu strains arise. Reducing opportunities for hybridisation of human and non-human viruses might reduce the number of highly virulent strains which appear, but wouldn’t knock it out entirely: we’d still need flu jabs.
Hmmmm… I think your claim of a food chain fully contaminated by excrement is a dubious one, unless you can figure out where you read that.
Hygiene does help prevent the spread of illness, so washing your hands, covering coffs and sneezes, etc. If you are wondering about the source of the virus each year, its origins in southeast Asia are likely a combination of climate and population density. This is discussed briefly in this article: https://www.scientificamerican.com/article/that-flu-you-caught-it-ca/
What I’m wondering is how a vaccine could be developed for that region. Flu shots in the US are based off of viruses present in asia many months in advance. Preventing these original illnesses would have a profound effect on health in the region, and throughout the world.
Just visit a rural Chinese village in Guangdong. In fact, in Beijing in prep for the Olympics they had a campaign to get people to quit letting their toddlers squat randomly in parks or any open space. many areas of China are like stepping into the 12th century in regards to technology and cultural ideas about biology and sanitation.
There has been some progress on this front. This is the region where IIRC, some important discoveries were made about human parasites with one or more intermediate hosts, like ducks or pigs and snails.
Also, in China there is a lot of live animal trade, both imported and shipped all over China. Live animal trade in the markets also mixes them up. All the flu variants that are normally isolated can infect more animals and “hybrid” viruses emerge, and people live intimately with the animals. We get swine flu, bird flu, the Spanish flu of WWI, etc.
And recall that Polio is transmitted by poop and contaminated entire lakes. plus the climate in Southern China is close to the body temperature of the animals.
I realise that giving it a nice sterile sounding name like “e. coli” blindsides the general populace somewhat, but the fact is, that California can’t even keep fecal contamination i.e. poop out of the lettuce and you’re questioning whether this seems far fetched in China.
This. The duck-pig-people cycle is real, and some idealized perfect sanitation regime could probably break it. But given that even the richest countries get outbreaks of something fecal sometimes…
Yucky anecdote time: visiting friends in LA, went swimming by Marina Del Rey, water tasted like poop. I went up to the lifeguard, mentioned that the water tasted bad, but I was used to the water down in San Diego, so maybe it was just different here? He said he’d test it anyway. By the time I got back to my friend’s place, the beach was closed for e. coli. Literally poop.
Surfers know better than to go in the water for a few days after it rains in San Diego because of sewer overflow. You risk skin rashes, etc. I got a bacterial pneumonia once. Or as I like to think of it — poop in my lungs.
So yeah.
Point is: Chinese cuisine consists of (exclusively?) steamed/boiled/fried vegetables, and with good reason.
Changes in lifestyle could have a big impact – in particular, not exposing ourselves to 1000s of others on the commute; an attitude change to take the day off if you think you might be sick (and so spare the rest of the office and train your virus); etc.
Research in the U.K. suggests that companies lose far more money to people coming into work when they should be off, than people pulling a sickie when they’re fine.
Enabling people to work from home is even better – not sure if you’re going down with something? Work from home, and avoid spreading it and feeling guilty if you turn out to be wrong.
Similarly, schools pushing attendance targets are also an issue.
The 1918 “spanish” flu killed 50 million. Some think it originated in the United States.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC340389/
Others claim the strain was already circulating in Europe before 1918.
https://en.wikipedia.org/wiki/Spanish_flu#Hypotheses_about_the_source
A healty organism (e.g. humans) is not one which never gets a flu or the like, it’s one allowed to react appropriately (e.g. with some fever, a day off etc.) to fight off the illness.
An HIV infected person kept in a clean room (meant: not getting in contact contagious vectors) also never gets a flu or the like. Doesn’t qualify as healthy either.
I refuse flu shots as long as my circumstances allow for and pay my bill in getting a flu every couple of years. I work with other colleagues in an EE/CS lab, do have 2 childs in school age and half a dozen pets in our flat + 2 ponies (not in our flat :^)
A real flu is not done with “some fever and a day off”. It’s one or two weeks of illness and high fever and can be live threatening. So it is of NO benefit, to get it.
He did have an “etc.” in there. I think that covers it.
Ivan J.I. thanks: yes, my “etc.” includes more. Let it be “few weeks off” as per flu requirements.
That said, I am not against vaccines to combat serious deadly illness (pest, cholera et al.).
Heck, I even have two VAXen in my ‘puter collection :^) a 3100/76 and a 4000/60…