[Gui Cavalcanti], whose name you might recognize from MegaBots, got on a call with a medical professional in San Francisco and talked about respirators. The question being, can we design and deploy an open source version in time to help people?
Unnerving reports from Italy show that when the virus hits the susceptible population groups the device that becomes the decider between life and death is a ventilator. Unfortunately they are in short supply.
The problem gets tricky when it comes to what kind of respirator is needed CPAP, BIPAP, or Hi-Flo oxygen NIV are all out. These systems aerosolize the virus making it almost guaranteed that anyone around them will get infected.
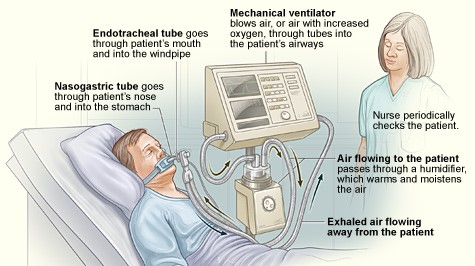
What we need is a Nasal cannula-based NIV. This system humidifies air, mixes it with oxygen and then pushes a constant stream of it into people’s lungs. If we can design a simple and working system we can give those plans to factories around the globe and get these things made. If the factories fail us, let’s also have a version people can make at home.
If you aren’t sure if a ventilator is something you can work on there are other problems. Can you make algorithms to determine if a person needs a ventilator. Can we recycle n95 masks? Can we make n95 masks at home? Workers also require a negative pressure tent for housing patients. This will be especially useful if we need to build treatment facilities in gyms or office spaces. Lastly if you’re a medical professional, can you train people how to help?
Let’s beat this thing. The ultimate medical hackathon begins.













Very basic but how about using Ardunio based microcontroller ..simple code could turn on/off a relay to drive actuator that opens valve for compressed air ( air compressor hooked upto oxygen tank somehow ..set to low pressure…hey ..plenty of them about ) to fill a mask / tube ….. ?? the electronics would not be to hard.. you need pressure / oxygen ?? maybe someone could expand on this if they see it usefull
First case of diy in the fight against the corona virus. A makerspace in Italy used 3d printers to create valves which the hospital ran out of.
https://mobile.twitter.com/michalnaka/status/1239316241984049152
There is a really good prototype from an MIT student published in 2010 where they build a basic vent for about $100. You could easily add the humidifier component to it, and other than that the only feature it lacks compared to standardly used vents is it doesn’t have the ability to account for PEEP. Google it.
I believe this is the project you are referring to?
http://news.mit.edu/2010/itw-ventilator-0715
And I believe adding a humidifier component to this would be a great addition – if their current redesign isn’t already including that.
This is just a load of chatter again, isn’t it? An excuse to get visitors to the site by picking on something that’s huge in the news. Have anyone at HAD contacted any hospitals?
If you can really help, it might be good to start up a group somewhere based on where you are geographically. Then you could phone the manager of a local hospital and ask if you could help. Prob be more difficult in the USA where people sue the people who are keeping them alive, for using an unapproved pencil to write on your chart. Ker-ching! It’s like winning a lottery!
This is 100% not the correct platform for a project like this.
Should start a subreddit
Hello, and welcome to Hackaday! We post links to and provide summaries of resources of interest elsewhere on the Internet.
Both of you: see the Facebook group in the first link in the article.
We are the map, not the terrain.
I have created a pubic-facing website, supported by a back-end collaboration website to enable engineers, makers and creators, medics and scientists to collaborate on this in a more structured manner. Please anybody message me if you want the details. I teach Systems Engineering at Oxford University in the UK and with the right help believe that we can make a contribution for everybody.
Can you please post the url?
Stephen Powelson did a 2010 student project at MIT for a low-cost emergency ventilator which is now being validated and redesigned for open source release within a couple of days.
http://news.mit.edu/2010/itw-ventilator-0715
When it is release they surely need volunteers all around the world to both source the materials and assemble them for nearby hospitals.
It might also be a good foundation for further development, to get it out there faster.
Can We Get a better organized thread going? Maybe a dedicated forum.
I say to 3d print as much as possible
ardruino for the brains
Everyone has connections 3rd hand or less to someone with a 3d printer and ardriuno.
I would be happy to put in some work on this, but unfortunately i have nothing more than a laptop and basic household items.
In 2008 around the time of SARS I looked into this whole area i.e. a minimum possible spec ventilator that used very little oxygen. It was a bag squeezer using industrial pneumatics. Our 2010 research paper seems to have been pulled from the listings just now when you look for it on pubmed.com (one there for conspiracy theorists) as it does have the word pandemic in the title but can be found here: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2044.2009.06207.x
I would design it differently now.
Initial Suggestions:
– Time is short, use an updated version of a tried and tested existing older electro-mechanical or pneumatic design. In the UK this might be the Manley, in the US something by Bird. The VW Beetle of ventilators if you like; reliable, people still remember them, made for ages, simple to fix.
– Machines proudly Made in Britain or indeed Made in the US may well contain many parts made in China, or even just be rebadged. Therefore simply “ramping up production” may not be possible. Check out the supply chains.
– For example, where would you find 20,000 pressure gauges with a range of 0 – 60 cm.H20 ? This is a very low range for any industrial gauge.
– Although Shenzhen is up and running, I suspect they are swamped with orders.
– Remember that veterinary equipment is often used human medical equipment.
– Would need to relax FDA testing rules.
– Would need to suspend opportunistic litigation against anyone using one of these in last resort situation, it would only be used as a last resort device and marked as such on the device itself.
– Needs to capable of being built using skills, parts and materials already available.
– Need to sublicense the design so can be built in competent machine shops and light engineering companies at a local level, no jealous guarding of IP.
– Huge organisational challenge. Needs heading up by the kind of character that gets things done bypassing all red tape. I am thinking of the ex-GM guy who organised liberty ship construction in WW2 or the Lockheed skunkworks mentality – did they not design and build a jet fighter prototype in 90 days? This person needs to be authorised to make decisions, facilitate the thrashing out of a design, then place the funding where required, instantly, with minimal paperwork.
“For example, where would you find 20,000 pressure gauges with a range of 0 – 60 cm.H20 ? This is a very low range for any industrial gauge.”
Yard sticks and tubing, it literally means the pressure to lift water 60cm.
Schrader valves in your car tyres measure pressure and temperature and transmit wirelessly. You just need to decode the frame. This has been done before using SDR
Got an accuracy and range problem there, they’re measuring pressures some 50 times as high as needed and they only have accuracy within a couple of PSI, which is double the maximum, so even used in a preloaded bladder/chamber or something to sense the difference outside if it, they won’t be any good.
Other car parts. This might bear investigating, I’m not overly hopeful about the sensitivity though. Ordinary 1 bar MAP sensors from naturally aspirated cars have a 5V supply and read ~4.5V at 1 bar, 14.7 PSI, that’s standard air pressure, they’re really for reading vacuum in the manifold. They will take up to 1.5 bar, another 7 psi, which will read ~4.8V… Now we need to read UNDER 1 psi, for a few tens of cm H20 pressure, so that’s a range of ~ .05 Volts over atmospheric. So we’re counting on a few millivolts here. Not ideal. We’d need a highly regulated, really nailed down no ripple 5V supply, then we’d need to mount an op amp circuit right on the MAP sensor, need to amplify that 0.05V mV range to a 0-5V range we can read with an ADC, and send over a longer wire. Opamp should be right on the MAP, everything soldered up to one PCB so we don’t get any fluctuations from contacts shifting, or stray EMI on long wires. When we’ve done that, we can characterise it and see if it’s even worth a damn in accuracy and repeatability, and how to calibrate it for changes in air pressure, and all that sort of fun stuff.
The statement in the intro that CPAP, BIPAP, or Hi-Flo oxygen NIV aerolise the virus and “thus is all out” forgoes that we may have the ability to adapt these machines.
So a second thread on the possibilities of adaption may be fruitful.
Other design and practical considerations:
1. Bear in mind that these machines are in widespread use.
2. Explain how this mechanically works out and how the virus gets earolised
3. Give recommendations to people who use these machines.
4. Design adaptions
5. Take in account that in the family home the chance of infecting family is significantly higher.
6. People (shall) live in lockdown a cpap look alike may not be perfect but very useful for a subset of patients with respiratory problems, given the scale of what is to come.
6. Adapting a tried and true medical grade machine seems to increase the likelihood of short term design succes increase significantly.
My two cents as a user of CPAP…
Kind regards
Onno
Is it not easier to fix outlet aerosolisation on alternative ventilators (and related devices) than build a whole new ventilator? I did this on a spitting airlift bioreactor by sparging the off-gas through disinfectant. You still get emissions, but they’re neutralised (I suspect here you could at least bring it below the levels of virus shedding from the patient) so long as the bubbles are small enough for good mass transfer and the residence time in the reactor is long enough.
I agree fixing the aerosolisation of CPAPs could be useful. One of the Doctors comments showed concerns of the mask leaking when a tee is used to filter the expiratory flow from a CPAP and hence the whole room is contaminated. Conceptually a soft hood or helmet or bag over the patient ‘s head with two tubes going through, one from the CPAP going to the mask and another coming from the inflated bag and going to @PorID’s neutraliser could allow the millions of CPAPs to be repurposed.
I think the solution has already been designed and built.
Besides the resurrection of “moth balled” vents, the MIT solution would be readily accepted by hospital staff.
The use of a manual resuscitator (hung at almost all bedsides) would be familiar to all staff. If the device could be made in such a way that ANY manual resuscitator could be dropped in and used, would be ideal.
The addition of heated humidified air/Oxygen mixture is easily added to the output or even the input side. I would suggest the output side to reduce condensation in the bag itself.
The exhalation side could have one of many bacteria filters added to reduce the risk of cross contamination.
Some alarms should be added in the event of functioning malfunction. This could be as simple as power loss or even low pressure due to disconnect.
Let’s get moving on this! Someone contact the MIT guys and get a set of plans and permission to build in qty.
As I stated before let’s pick a plan, decide on where to send parts, and get moving.
https://www.projectopenair.org/
I am rapidly building a collaboration network of engineers, scientists, innovators and people with skills in building and making to help address the need to build ventilators. I absolutely applaud your ideas and effort here and would like to invite you to join this community. To be clear – this is a not-for-profit endeavour. I teach Systems Engineering at famous British University (your favuorite search engine will find me).
Control-System Engineer (Physics graduate from Imperial, when rated) working on novel decontamination idea(s) ~ basing my tech on cat coronavirus, which suggests this is here for the long-term, not just April :-(
However, I would suggest off-the-shelf hacks using medical / food-grade kit, and keeping 3d-printing to essentials like holding / merging specialist parts in place. Having spent quite a while in Home-Brew syphoning , clear silicon tubing will soften up in warm water (bucket containing spirals). So you could stroke an array of tubes it from outside (rotating bumped wheel), like a Peristaltic-Pump. So you have warm air in a moist environment. You can store this extra pressure in an array of soft-drink bottles. They are clean(able), able to take pressure, and voila have a screw thread to a manifold-array (albeit various styles which need help of 3d printer guys). Screw in array of soft-drink bottles and bodge with some fish-tank? compound.
You need temperauture and humidity monitiring ~ chips to 1% are available.
Your most accurate cheap pressure gauges are going to be water height or bellows, even a webcam on balloon inflation.
You need THREE different software engines (‘cos this is a bodge), and come to a consensus view. Maybe cheapo 24V industrial controller, 12V engine-management (maybe Arm), Raspberry-PI(x) ~ at a push, add on cloud-monitoring via AWS or Azure portal ~ You need ALARMING of strange conditions. Think SMS text to Nurse Wiggle, Bob’s machine aint working right. On dangerous condition, need to back off. Don’t burst their balloon. So ideas about extra mechanical safety release are good.
One of the problems I read about is the shortage, but the inefficiency of Y-tubing the respirators for multiple patients. Is there a better chance of designing a software patch to test the resistance and compensate accordingly?
I found this project by MIT that created a $100 homemade unit comparable to $30,000 unit. Its simple, but its something. We should get the designs from the authors.
https://www.fastcompany.com/1661942/mit-students-invent-100-ventilator-for-disaster-zones
DIY version that could be improved on
https://www.instructables.com/id/The-Pandemic-Ventilator/
What if we instead look to the past, I am sure this is easy to replicate:
https://apps.dtic.mil/dtic/tr/fulltext/u2/623457.pdf?fbclid=IwAR3PWtrosNOLBqpcWhFFWhr-x1kKI665hpEAAvxCC3TJnWWc1fKJJTEyWjY
Google search “Army Emergency Respirator” from WW2
The ventilator is already done by MIT students using arduino. https://www.fastcompany.com/1661942/mit-students-invent-100-ventilator-for-disaster-zones
I hope a really good literature search is being done by someone in the group. No point in “reinventing the wheel.” There was a MIT project in 2010. http://news.mit.edu/2010/itw-ventilator-0715. Perhaps there has been further development since then.
Is there any way we could hook one machine up to multiple patients?
https://mobile.twitter.com/alandrummond2/status/1240008793167192066 Like this?
I just found an interesting sample design on the NXP website: https://www.nxp.com/docs/en/application-note/DRM127.pdf
I have 3 CR-10s and enough filament to get started. Please let me know how I can contribute. I have these set up to mass manufacture so we could start pounding out parts almost immediately if need be.
What about this low-cost arduino-based ventilator?
https://github.com/jcl5m1/ventilator
The only benefit of a ventilator is if the patient cannot breath for themselves. Why can’t we deploy the millions of prescribed CPAP machines to help patients not get to that point? Nothing new to invent, or manufacture. No oxygen needed either. Just collect CPAP machines so hospitals and clinics have an entry level breathing aid, and can reserve the ventilators for those that really need them. The other bonus is that most CPAPs include a water reservoir to moisten the air. And, one thing that immobilizes a virus is humidity in the air. Seems to me that Americans millions of CPAP machines could be a positive improvement in caring for Coronavirus patients, before they require a vent to breath for them. Am I right?
Here’s a design spec for an older design Incase it wasn’t already posted. https://www.nxp.com/docs/en/application-note/DRM127.pdf
“Can we make N95 masks at home?” – Yes, it is possible. How can I submit a proposed solution?
Moody,
That would be a superb contribution if inexpensive. not enugh masks now for general use.
steveb M.D.
Hi Everybody, I also started thinking on the same concept, and made some trys.
I am new here, thanks for your indulgence and advices.
My work is here: https://github.com/berniv/diyRespiratory
The specification I want to reach is like CPAP / BiPAP / PEEP: pressure of 5 to 15 cm H2O, cycles with 2 pressure levels, flow high enough for breathing. Also very easy to manage without measuring instrument.
The proof of concept are now at this point:
1. Air pump made with 3D printed things, RC motor, wood plate: ok, pressure obtained 6 to 10cm H2O depending air flow
2. Measuring pressure with syphon, simle and no need instrument
3. Arduino clone to manage cycle and check pressure level with wires plunged in the syphon
Now the remaining work for continuing PoC:
4. bring the air to mouth (create mask, connect with tube)
5. manage exhaust, my idea is 2 levels of pressure, using a servo
6. filtering air and adding moisture
7. adding an interface to manage the pressure levels and cycle time
8. adding separate cycle checking and alarm in case something is wrong
i think using a turbine is going to cause a probleme in the following points (keep in mind that the patient needs a controle on the air volume as well as the pressure):
1- controle of the flow rate. since it’s a rotating machine there is a delay in the stoping of the motor and the stop
of the airflow.
2- the flow rate has to be constant over time.
3- The patient needs only a small amount of air, to my opinion it’s going to be too much air flow with the turbine.
4- and most importantly the pumping in devaice has also to pump air out of the lungs, wich is going to be difficult
with a turbine it will have be with a 3way valve or somthing in that kind and a complicated piping system.
i think we should use a constant volume pump such as an (Ambu bag) (in French: Ballon auto remplisseur à valve unidirectionnelle). with a mechanical system of compression such a chain link or a 3D printed Rocker arm system
i strongly recomande this papaer, it dates to 2010 but i’m screening for an update, let’s keep in touch for the following:
https://web.mit.edu/2.75/projects/DMD_2010_Al_Husseini.pdf
Nor sure if this has been shared already; https://www.instructables.com/id/The-Pandemic-Ventilator/
Medical people, Is this close to the Minimum Viable Product (MVP) for what is needed?
Does anyone have access to these drawings/blueprints mentioned here; https://www.theguardian.com/business/2020/mar/16/vauxhall-owner-psa-car-shuts-european-plants-amid-coronavirus-fears
That should save us some time.
I’m in South West UK and have good links to manufacturing and willing to help.
RE: These systems aerosolize the virus making it almost guaranteed that anyone around them will get infected.
Could the exhales, be passed through/bubbled through a chemical, like meths or ethanol to sterlise the outgoing breaths, or like passed through boiling water to sterlise
I am retired from Respiratory therapy, started back when we were called Inhalation Therapy, what about exhale (another story). With more than 30 years in the field.
If someone brought the MIT Vent into the hospitals where I worked I would immediately know how to use it. I can safely say that 99% of Therapists, Nurses and yes even some Docs would see it and say yup that will work. They would be able to connect to humidifiers, bacterial filters and even PEEP/CPAP devices and monitors. O2 blenders are available to dial in ordered FIO2.
It is a simple device made from almost all parts purchased from Ace Hardware/Home Depot or Lowes. The stepper motor, arduino and a few other parts may have to be mail ordered.
The heart of the device AND what makes it so attractive is that it uses a manual resuscitator bag. As I have stated in a prior post these are located by every bed in ER and ICU.
Here is a link to the paper from MIT:
https://web.mit.edu/2.75/projects/DMD_2010_Al_Husseini.pdf
The size of the bag can be adjusted from Adult to pediatric.
This is what direction I think we should be headed. Fast build, Resuscitator Bag already medically approved and the whole thing can be sterilized to be used from pt. to pt.
Some people have commented such a device might aerosol the virus on exhale.
As somebody with experience do you think this would be a real issue in the current situation?
We will quickly move to emergency medicine with patients in special hospitals or tents as the numbers go up exponentially so cross-contamination with other patients will probably one of the lesser worries.
What seems to be the most pressing issue right now is that without a ventilator the outcome is almost 100% certain while even a simple solution might increase survival chance.
No filter is 100%. But almost every med supply chain carries some or all of the existing filters.
https://www.medtronic.com/covidien/en-us/products/mechanical-ventilation/filters.html
Can CPAP machines used for sleep APNEA be reconfigured/repurposed in some way?
I called a manufacturer of CPAP machines and asked. The short and official answer was they could not be used,
a firmware update won’t do the job anyway.
For sleep apnea it’s a pressure range typically between 6 and maximum 20 mbar. A typical value for ventilation is 35 mbar. If two cpap machines, that is, their blowers, could be coupled in line this might supply enough pressure for many cases. I guess it would require a lot of reenginering and modifications and then still end up as a complicated and unreliable system.
Hi all. There is a group people doing the same in Spain.
At the same time we are trying to make things useful for the people at hospitals, like face masks, respirators or spare parts for when normal distribution can’t reach.
https://foro.coronavirusmakers.org
Why can’t we rejig – the CPAP machines out there… We have a lot of CPAP machines – commercially available too… the only thing is to ensure that the CPAP machine does not aerosolize the virus particle. That might be an easier challenge to solve than to completely reconstruct a new Ventilator from scratch… or at least buy some time until ventilator production at scale can be achieved in some companies. Also newer models of CPAP come with thermostats and water units that in essence do what the Nasal canula based NIV is doing – or have I understood something wrong?
How about using a smartphone (and app) as a device for measuring and controlling? They often come with many sensors: Barometer, Magnetometer, Acellerometer, Gyroscope . Signal outputs might be possible by the headphone jack, e.g. to send pwm signals to RC-servos.
Needs a RTOS or dedicated microcontroller. In theory, you could validate a RTOS replacement firmware for a fixed set of phone hardware, but not in the timeframe that would be useful and not for more than one phone model per effort to do so. You could get it to log and measure stuff, as general nice to know how the patient is doing info, but don’t for goodness sake put it in any feedback loop.
This is a device that can be made with off the shelf parts or a modified CPAP with oxygen infusion. ?
Experience in design, fabrication, firmware, software and electrical engineering, including pertaining to medical devices.
Most pertinent skills: Circuit and PCB design, firmware/software for any embedded platform, all Arduinos, ARMs and RPi’s.
I have a machine shop and EE lab. I can do rapid prototyping in metal, plastics and composites and casting/molding silicone/urethane rubber/urethane plastic. Also, rapid circuit design and programming.
Direct email: corona@ericsinger.com
I saw this on another site. Maybe you could discuss it with him.
https://hackaday.io/project/170434-simple-ventilator-air-supply
I wanted to get this idea out there and see if it sparks anything in anybody else or passes basic muster with someone in the healthcare crowd
https://hackaday.io/project/170434-simple-ventilator-air-supply
Seems like someone is already working on a solution:
https://www.notechmagazine.com/2020/03/open-source-breathing-ventilators-covid19.html
For the valve at the mouth could one use a simple tesla valve on both ways to alow exhalation out and fresh oxygenated air in? The advantages are that it is an easy shape to 3d print, and can be made with no moving parts.
here is the link to a basic ventilator valve using 2 tesla valves
https://www.tinkercad.com/things/hoiXE781ceX-oxygen-ventilator-valve
The problem gets tricky when it comes to what kind of respirator is needed CPAP, BIPAP, or Hi-Flo oxygen NIV are all out. These systems aerosolize the virus making it almost guaranteed that anyone around them will get infected.
Is there any chance we could put a trap on the exhalation line to catch the aerosolized virus? Vacuum supply companies have a range of mist eliminators and other traps designed to catch particulates in a system’s exhaust. See here for some options.
CPAPs are safe and fairly common, so a way to leverage them toward emergency needs might be very helpful. Much less so than an ICU, obviously, but in the middle of a pandemic we may have to do our best with what’s available.
Doctor Dayo Olakulehin of Nigeria several years ago invented and produced a mechanical ventilator he called D-Box. I do not know if the ventilator received certification or if it has application for the support of COVID19 patients. The principle of D Box appears to offer an example of effective innovation toward a design which maybe quickly produced , replicated and developed. I will leave aside here consideration of proprietary issues which may apply.
Details of Dr Olakulehin and D-Box may be Googled.
Would it be possible to modify a CPAP machine to perform this function? Add some oxygen to the air intake with a valve and let the CPAP do what CPAP do?
Real Technical Specifications from an emergency collaborator can be found here
https://docs.google.com/document/d/1FNPwrQjB1qW1330s5-S_-VB0vDHajMWKieJRjINCNeE/edit?fbclid=IwAR3ugu1SGMsacwKi6ycAKJFOMduInSO4WVM8rgmC4CgMJY6cKaGBNR14mpM
Existing projects can be found here: coronavirustechhandbook:
https://docs.google.com/document/d/1HRrUwpSi63hV8UqEYumJZ29v8obkdWyQW0QgOiybgrQ/edit#heading=h.2bjxomvr7fcz
Apart from personnel to operate the devices, also disposables for these devices will run out (dixit Belgian health officials). If you have more information about what exactly these disposables are, their specifications or how much will be short (when, where), please add to this forum to track shortages and tech specs, to guide the community in their solving efforts:
https://gzt.be/covid19-breathing-machine/forums/
We have experience working on ventilators. If you want help with the control algorithm for the ventilator, please email me at ventilator@smartr.ai. We would be happy to help out.
If you need to use a PIC or a raspberry pi anywhere in this I can do the software for you.
maybe starting from existing cpap/bipap machines might get there quicker
I’ll see what I can do design wise (I work In a prototyping company) we have 3d printers standing idle that companies don’t want anymore (fdm) I believe I can design something using some simple valves and 2 belows powered by stepper motors and I have a work colleague who’s partner is an NHS ward manager so I’ll put something together and ask
What needs to be achieved from what I can see is controllable air volume, controllable breathing rate, a way to warm and moisten air (bubbling air through warm water) ability to both push air into lungs and out.
Honestly, while an sutomatic unit is definitely preferable and a worthy project, perhaps first focusing on a hand-powered unit would be best, such can probably be 3D printed with minimum additional parts required.
Millions of Americans use a c-pap for sleep. Could it be possible that they could be modified and used to free up ventilators for people without them?