[Gui Cavalcanti], whose name you might recognize from MegaBots, got on a call with a medical professional in San Francisco and talked about respirators. The question being, can we design and deploy an open source version in time to help people?
Unnerving reports from Italy show that when the virus hits the susceptible population groups the device that becomes the decider between life and death is a ventilator. Unfortunately they are in short supply.
The problem gets tricky when it comes to what kind of respirator is needed CPAP, BIPAP, or Hi-Flo oxygen NIV are all out. These systems aerosolize the virus making it almost guaranteed that anyone around them will get infected.
What we need is a Nasal cannula-based NIV. This system humidifies air, mixes it with oxygen and then pushes a constant stream of it into people’s lungs. If we can design a simple and working system we can give those plans to factories around the globe and get these things made. If the factories fail us, let’s also have a version people can make at home.
If you aren’t sure if a ventilator is something you can work on there are other problems. Can you make algorithms to determine if a person needs a ventilator. Can we recycle n95 masks? Can we make n95 masks at home? Workers also require a negative pressure tent for housing patients. This will be especially useful if we need to build treatment facilities in gyms or office spaces. Lastly if you’re a medical professional, can you train people how to help?
Let’s beat this thing. The ultimate medical hackathon begins.













And it all comes down to this – you can create anything you want but in the USA it will never be used do to restrictions on medical devices. You can make the best thing in the world but until that goes through thorough testing and passes all the government checks and balances, it is just a paperweight.
For down the road or for developing countries that don’t have tight medical restrictions, sure, but for the USA you are living a pipe dream.
https://www.facebook.com/groups/670932227050506/permalink/676507283159667/?hc_location=ufi
Pipe dreams are not killing people. Strict Rules that do not fit the circumstances of a crisis often do…
True dat.
Not really a pipe dream, for instance you can build a geodesic dome for practically nothing,, cover it however you wish add ventilation and you have single unit structures or ward like structures. Has it been done ? Not yet, are they legit structures? absolutely .
Think of a igloo for example, tunnel door, Ppe doffing area, another sealed door to patients, I’ve seen these things, they can be as big or small as you want to make them, they can be permanent or temporary.
Just because something hasn’t been done yet, doesn’t make it a pipe dream, afterall Nikolai Tesla theorized about Wireless current powering the world, While it’s not exactly the same our wireless connections validate his work.
Keep on bouncing ideas , nothing lost by sharing thoughts, everything is gained if we hit just one idea that is realistic and feasible
Before writing everything off as a pipe dream,
Go to the FDA emergency authorization web page to see what authorization you need.
https://www.fda.gov/medical-devices/emergency-situations-medical-devices/emergency-use-authorizations
Yes – there are exemptions like that in many jurisdictions.
BUT – they dont apply to home-made devices built using parts from the hardware store.
If you look at the exemption …
’emergency use of ventilators, anesthesia gas machines modified for use as ventilators, and positive pressure breathing devices modified for use as ventilators (collectively referred to as “ventilators”), ventilator tubing connectors, and ventilator accessories that FDA determines meet the criteria for safety, performance and labeling’
In other words – machines that have already been certified for a particular use, to be MODIFIED for deployment as a ventilator – and MEET THE REQUIREMENTS FOR SAFETY, PERFORMANCE AND LABELLING.
MODIFIED – not built from scratch in an unregulated environment with no quality management system.
In other words, these machines need to be certified already, and MODIFIED by experts that understand the physiology of sick patients and the medical device/quality management standards.
Now if I could save an individual life by using a vacuum cleaner and a plastic bag, of course I would.
But that isn’t scaleable, and doesn’t fit the exemptions under FDA rules.
The Uk spec for building ventilators is published here
https://www.gov.uk/government/publications/coronavirus-covid-19-ventilator-supply-specification/rapidly-manufactured-ventilator-system-specification
The effort on this thread is truly admirable …
But we need to think more broadly than trying to build a home-made ventilator.
This approach will NEVER be able to scale to meet the demand for devices, training, support, sterilisation, consumables, maintenance etc – and will never be given the types of regulatory approvals needed for use in hospitals.
Deficiencies in design could very easily kill more that they save, particularly because (like 100% of the home-made attempts Ive seen) they dont consider the design elements necessary to prevent healthcare workers becoming infected.
If HCWs are exposed to the virus through poor ventilator designs the dont control virus-laden aerosols, HCWs will become patients, leading to the collapse of the healthcare effort and >> INCREASING FATALITIES <<.
Existing manufacturers are scaling massively and delivering certified, supported machines through established distribution channels.
Example here from ResMed …
https://newsroom.resmed.com/news-releases/news-details/2020/ResMed-Statement-on-COVID-19/default.aspx
What we should be doing in this hack is focussing on ways to support their supply-chains, and managing spread of the virus to PREVENT disease, rather than trying to treat it by attempting to build a complex machine ourselves, with insufficient knowledge and no experience.
I’m sorry, but does this even make sense? Can’t we just buy the plans for an existing design and open-source it? Surely a philanthropic corporation and a philantrhopic mega-donor could get together and make this happen? Woudln’t it be a much better use of time to simply purchase an existing design and start mass production immediately? Perhaps modify it if we can’t get certain parts? This is a solved problem, probably solved multiple times over, re-inventing the wheel with so little time available seems like a poor use of that time.
This is a good description & existing invetions.
https://docs.google.com/document/d/1HRrUwpSi63hV8UqEYumJZ29v8obkdWyQW0QgOiybgrQ/edit#
Also check this out https://www.facebook.com/groups/670932227050506/permalink/676507283159667/?hc_location=ufi
PLEASE READ: The device described it a high flow nasal cannula system. THIS IS INAPPROPRIATE at this time for treatment of coronavirus. Most patients requiring any pressurized NIV go onto needing intubation and ventilators regardless, and NIV increases the risk of aerosol transmission, and is not being advised for use during this epidemic.
Please refocus efforts onto creation of an actual closed circuit ventilator.
Thanks,
Brad Green MD
For less severe cases, could someone’s own CPAP or APAP be fitted with tee fitting to connect an oxygen tube (with some form of flow control) to help them? Maybe that could keep real ventilators available for more severe cases only.
Maybe its best to see what is being coordinated and assist with the project based here
https://www.3dprintingmedia.network/3d-printing-unite-for-covid-19/
Is it possible to hook up 2 patients to one ventilator (if so , for which type of ventilator)?
because that would double the capacity *and* build on tested/approved apparatus.
NO! But a good question. :)
Masks for people, not medical staff could be created DIY it seems: https://www.youtube.com/watch?v=aNjpH5lBZ8w
A bit of a different approach. Manufacturers of non-medical equipment
The right amount of equipment can be produced by other manufacturing enterprises.
Probably need old models. Why? Other manufactures are not specialized in this kind of equipment. Many modern technical and technological solutions on their basis will be difficult and long to implement. Although a lot of medical equipment was developed decades ago and has passed several generations.
In such cases, technical and technological documentation is needed. I will separate the manuals, various repair and maintenance instructions, and training materials.
Where can I get it?
– Ask the manufacturers’ companies. They can store documentation for older models;
– Old companies. The documents could have been saved somewhere;
– Organizations (both private and government) that certify and approve equipment. In many countries, they require complete documentation for a decision;
– Customs
– The services for export/import control;
– Some documentation may be available from companies providing equipment maintenance and repair;
– Some information may be in old patents;
– In libraries and archives.
Commercial and law aspects of the problem
Medical equipment requires serious testing and certification. This is usually a slow process. That is before you start doing anything, it is better to coordinate the procedures with local regulatory offices. They will explain many of the details, etc. Perhaps they will agree on a simplified procedure. For example, it works in the current situation and then the equipment is taken out of service before all the procedures have been completed.
It is possible to agree with owners of intellectual property on various licensing, support and sales options afterward.
Yes, it is understandable that in such situations even laws are on the side of those who do (see the law concept of necessity), but people are much more likely to be contractual when they understand that they too will benefit.
Training
A very important aspect. All medical equipment works with people. And if it’s done by the rules, mistakes in use can be harmful. And serious harm. Even death. The moment of training has to be agreed upon first. Because need people who can understand how to use this equipment and teach others.
What kind of manufacturing can be suitable for the level and culture of production? Aviation, space, underwater vehicles, some automotive, cosmetology (equipment, not service) and the like.
I have worked on numerous ventilators and have some recommendations. Not an engineer, just a BMET. First of all, not all sites have access to medical gas. Some old but very reliable units at one of my sites uses a blower very similar to a draft inducer in a furnace. You can adjust to voltage delivered to the blower to adjust its output, and it delivers a constant flow. Three valves control the flow towards the patient. One is for oxygen, one for air, and one for pressure.
The valves are not identical but all of the flow sensors used to control/calibrate the unit are the same. The pressure in the circuit is controlled by opening a closing a port which goes back into the unit (the more the valve closes, the higher pressure you get in the hose) which allows the continuous airway pressure to be adjusted. Overall, it is three valves and three flow sensors with an external oxygen sensor which is not even needed for the unit to run.
Maybe some stepper motors, valves, and electronics or even potentiometer for adjustments? Every place with enough qualified people is going to have a BMET available to help calibrate and test machines to ensure they are good for patient use. Even if the machine is checked and adjusted after every patient it could maybe help keep the design simpler? A lot of hospitals will have access to tanks of oxygen but out of all 9 of the sites my team works at only one has a single tank of air. If units are set up in hotels and such temporarily it might help to use one that does not require external air delivery.
Haven’t read all this yet, but I have three items:
1. What is the difference between a respirator and a ventilator?
2. Can you make DIY Oxygen? You need oxygen along with the ventilator, right?
3. There is NOTHING new under the sun:
https://hackaday.com/2007/05/25/diy-powered-respirator/
Check out the YEAR of that post.
The fact that there are THOUSANDS of “hackers” and makers out there confirms my belief that if government would just get out of the way, INDIVIDUALS as part of NON-government organizations will handle the pandemic better than government.
Doubt me? Ask the simple question: WHO (pun sort of intended) caused the problem? The answer is: GOVERNMENT and the red-tape they created and in many cases the lies government told.
Why not allow people to try whatever crazy “natural” remedy they want to? I’ve seen several articles about people (doctors?) trying stuff like “arthritis medication fights coronavirus”. I can’t remember if that is one of the actual headlines, but they were that weird.
How does this device compare with an oxygen concentrator?
Is anyone project managing this? I feel like if the design using easily available products from home Depot, or a hardware store it is even more deployable.
I would like to help, I have many responses for coding, and microcontrollers and hacking hardware together for fabrication. Can also build and test designs.
I am located in nyc
Im not sure who is pmíngthis but there appears to be something coordinated here
https://www.facebook.com/groups/670932227050506/permalink/676507283159667/?hc_location=ufi
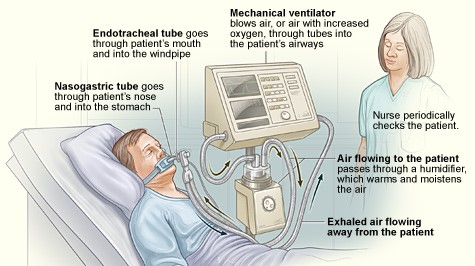
“Nurse periodically checks the patient”
Nurse is falling asleep standing up due to staff shortages and has no PPE – pic is too real :(
Dumb question — but do you think there is a way to leverage “out of commission” CPAP machines to get at least part of the way with a hack? Many of these are remotely programmable…. not sure if there was any other thread that posted the idea — I’m new to these types of forums, but didn’t see this put out there yet…..
Well its time for America to do what America does best, Innovate. The medical industry has done their very best to strong arm all medical tech out of the reach of anyone not in the “club” but the time for that is over. If we act now we can 100% build a better mouse trap than those clowns selling $11,000 respirator valves that cost 10cents that they can’t seem to produce. Based on the information provided we should look at moding OTS (off the shelf) where ever possible. I believe we can fairly easily Mod full face snorkel masks to provide the closed circuit we are looking for and the back end does not sound very complex compared to what many of us do day to day. Ive got 6k sf of work shop, 3d printers and am ready to get to work.
https://docs.google.com/document/d/1HRrUwpSi63hV8UqEYumJZ29v8obkdWyQW0QgOiybgrQ/edit#
https://www.reddit.com/r/CoronavirusUS/comments/fkt3uk/louisiana_selling_ventilators/
Louisiana is selling older ventillators. These are likely broken/partly decomissioned but may prove useful for reverse engineering.
This is a interring project https://youtu.be/0386hOgcQTA
Please note that the tube has been exceeded, you have to ensure that the rebreathe of CO2 is not to high, since the tube is extended.
I am thinking of using a tier inner tube to press the Rubin balloon. The tier inner tube inside av PVC pipe together with the manual balloon. The tier inner tube is inflated using compressed air. Timer relay and a magnetic valve controls the breading cycle.
We just need somone to take the lead, the skills and resources are here.
I’m thinking of putting a Ruben balloon in a PVC pipe together with the inner tube for a tire. Timer relays and solenoid valves inflate the inner tube with compressed air. The relays control the breathing rate. Here is a similar project https://youtu.be/0386hOgcQTA
This FB Page maybe useful
https://www.facebook.com/groups/670932227050506/?notif_id=1584558656671241¬if_t=group_r2j_approved
Is there a design here somewhere?
Not sure if this has been thought up yet but a SCUBA regulator is essentially an early ventilator. There would be a lot of issues as it would be very limited in application but it would be better than nothing.
Has anyone moved this to a more organized setting? Is there any information on organization? what resources are needed? I have a couple of servers in my lab that are not running and I want to know how I can help.
I posted that on facebook. It is so important to get organized. Maybe some page. I can make one for tomorrow morning, but then people will copy that and make a new one. It needs to be 1 global page about items that are available and resources that are needed. Government is not interested in talking with us. But we cannot make 10,000 pages and 1000 models of ventilator valves. I love your project guys. It is a good start.
Let’s don’t make 1000 the same ventilators.
And it is not that it is not happening already. It is up to you if you want to help or not.
I send email to my practice asking to pass it to someone who deals with supplies. To give them my number and email. Just in case.
We don’t need it today here in England and kids go to school tomorrow. England. But we have now the opportunity to team up, get ready, get the parts done. And I wait for the phone call, that pray will never come.
I am taking this approach. I have a Medial Doctor that works with me as I work with him on another project. He has contacts in Hospitals in Łódź and Bytom in Poland. If you live in this area and you have a 3D printer you can drop me a message and we will be on “Stand by”. The word is currently spreading.
Let’s get the files ready and sit and wait for orders from people who know what they are doing.
I will have pictures of the mask with filter M95. I also asked to help us verify our designs. There is no hospital in the world that will use them if they are not safe.
Now we have time. Let’s get ready, but don’t start printing yet.
https://hackaday.com/…/ultimate-medical-hac…/comment-page-2/
I have 10 Arduino at home and 1.5l of resin. I could make 5 of them. I just need help, as I honestly don’t know much about ventilators. I was helping Doctors with the Medical Software to issue the medication, but this is a new challenge for me. 3,5 years as a Software Support Consultant for British NHS. I know them. They are amazing. Let’s help them a little.
Mostly, to just boost morale.
https://web.mit.edu/2.75/projects/DMD_2010_Al_Husseini.pdf I found something in the internet from MIT. But the description is not very detailed. It is from 2010.
Guys. I have 3 or 4 pumps for dispenser. If you turn them on they pump air. I have 5V and 12V that could work as a pump. For the computer I have a range of Arduinos. 20. And 2 Raspberry Pi.
I just bought a 3D printer and I have a range of tubes and connectors. I can make it myself at home. I am keep getting told of when I mention making parts in 3D now only to get ready, as I apparently don’t know nothing about it.
Well. 3,5 years as a Software Support Consultant. Degree in IT and Games Design. At the back sit is a Medical Science Doctor that supervise me.
I probably may not need it in UK, but I will start making one, just in case. I am a First Aider and everybody is concern about the medical certificate on it. I don’t think that the wife of my collapsed neighbour, would be asking me if it is certify, if I will be performing a CPR on him, by myself. As the ambulance cannot arrive for 30-60 min. I don’t know if anyone did CPR in life. I didn’t. I did it only on training and it was already tough. I would rather focus on his hearth to keep it running, then on both.
I am start designing one that is based on the parts that I have currently at home. I even have buttons and LCD screens to change the values of it how it works.
I really hope that I will never ever have to print it. But I want it to be ready. At the moment the professionals are doing the job. I will leave it to them. But I want them and public to know that it is not only them that they can count on, but one all of us. We need to help each other. We forgot how to do it, so lets bring it back.
Hi all just wanted to share these docs on some related info.
Specification: https://www.britishchambers.org.uk/media/get/Specification%20For%20RMVS%20Challenge.pdf
https://gitlab.com/TrevorSmale/OSV-OpenLung
https://app.jogl.io/project/121
If anyone wants to help: https://www.projectopenair.org/
Nice looking website. How do we use it to make things happen?
Hi, As for O2 concentration, please watch this video “John video 9” @ 22:48 from Dr John Campbell.
The patient infected with COVID19 required 2 liters per minutes of oxygen, for 3 days, dilivered by nasal cannula:
“John video 9”
https://youtu.be/9W4zyQ_dqxI?t=1368
2 Lpm, not 22 or the other numbers some have posted above
2 Lpm by cannula
A critical component of the ventilator is the oxygen generator. Is it possible to use the oxygen generators and tanks used in the emergency oxygen system in jetliners? These devices are capable of providing O2 for about 15 min. So:
(1) Can the generators be configured to generate longer?
(2) If not, is it possible to use tanks be used to store O2 while the generator is idle or cycling the next supply?
After all, Boeing has almost 800 737 Max 8 grounded, each having more than 200 emergency O2 units. At 15 min. each this total to 800 x 200 x 0.25 hr = 40,000 hrs. (approx.) And that does not count all the other hundreds of jetliners that sit idle in airports all over the world.
Another component is preventing the exhaled air from contaminating the environment. (This is part of making the device medical grade.) Since the exhaled air contains a significant portion of O2, it (the exhaled air) is recycled for breathing in closed scuba systems. I suspect that this is done by ventilators as well, because there is no concern with a patient re-breathing their own exhaled air. But, of course, most of the air must be eventually expelled or scrubbed.
Preventing the exhaled air from contaminating the environment can be done by other means then internal to the ventilator. A patient, who is ventilated with a ventilator that is not protecting the environment from the exhaled air, can be placed in a negative-pressured tent, the air of which is filtered.
????
Ventilator for rapid response to respiratory disease conditions
Canada Patent CA2666337C
https://patents.google.com/patent/CA2666337C/en?q=emergency+ventilator&oq=emergency+ventilator
Patent abstract:
The present invention relates generally to the field of ventilators, and, more specifically, to a ventilator system that addresses respiratory distress due to the onset of an epidemic or pandemic disease state. In particular, the present invention is a ventilator system that can be manufactured quickly with minimal skill requirements and employed rapidly in response to epidemic respiratory disease conditions.
Hello all. I own a CNC Machine shop and steel fabrication shop. We also have an electronics department where we automate our mechanical-motion fixtures and integrate them into our CNC machines. I would be happy to develope anyones’ idea of a practical design of a resperator. And we also have bottles of oxygen for our Fab shop that we can use for the project. Lets stop talking and move on to Doing.
Russ Lanphier, First-off CNC products
We should all band together, purchase this company, and scan these parts so we can print out molds with 3D printers, so we can save our families and neighbors. Here is an exploded diagram of probably the best respirator. https://percussionaire.com/products/phasitron So, if you read more on the site, and what this respirator does, it is exactly what is needed after a corona virus has ravaged a pair of lungs. Keep the lungs open, remove sputum, get oxygen in, remove carbon dioxide, without damaging the lungs. This guy, Dr. Bird, spent his whole life inventing respirator after respirator. This is not something we can engineer in a week. But if we could license the design for $100 or so per person, we would have a license to print out a copy of what they’ve got. So, we should all band together and purchase this company.
lwe should be building more ventilators NOW. i woul gladly volunteer. Give current ventilator companies a royalty for their designs, specs and expertise. We can save more lives. It is not rocket science.
I would love to lend my skills to this project in any way I can. I have a decade of experience designing 3D-printable mechanical devices and working with electronics. I do not, however, have any experience in biomedical devices. If someone out there does, and wants to collaborate, or can point me to somewhere I can be of help on this matter, please let me know.
http://bryancera.com
Ok I just saw a design with an Ambu bag. Brilliant!!!! So two things are important. The amount of air displaced by squeezing the bag must be adjustable from very little squeeze to full collapse squeeze. Also the rate of the squeeze cycle needs to be adjustable. Does anyone know what is a typical breath rate range is spanning from children to very healthy adults?
Are there any projects started which could use help from a programmer who doesn’t have a medical background?
Always looking for ways to put my skills to use for the world, but for this specific situation I’m not quite sure where to start looking.
I apologise if the answer is in the facebook link from the article, I don’t have a facebook account so I can’t view that page.
How about using an internal combustion engine for negative pressure suction? I can hardly imagine any virus surviving the trip trough it. Only thing i could imagine was any air leak in the connection leak between a turbocharger and the air intake of the engine. Think about negative pressure tents/cubicles in that context.
When calculating the volume of the engine times its rpm (and then i think divide by two in case of a four stroke engine) it would be one cubic meter per minute for a typical car engine at 1000 rpm.
The somewhat higher pressure from outside of the cubicle could then be employed to drive or boost various setups for breathing assistance.
I can not asses that, could maybe inside a negative pressure cubicle some of the patients use masks instead of intubation?
One more thing: Blood co2 levels seem to be a problem also, so how about purifying the air from co2 before it’s going to the patient? They devlope those direct air capture technologies for large scale by now. Would it make a difference to have e.g. 150 ppm instead of 400?
There is a new and very low cost humidifier that can be used in a cannula-based NIV, a Flash© humidifier.
It costs about $20, a fraction of the price of other humidifiers, and it is much safer because it evaporates water in 1/100th of a second, leaving no droplets. It has no standing water and cannot grow pathogens.
I am making these new Flash© humidifiers right now. Contact me!
Aryeh Tench
Founder
Snapp IP
So if you blend x% of Oxygen with x% of compressed air is it ok to deliver this direct to the patient or would you need to warm this mixture and would you be better off bubbling this through water to add humidity – sorry and what % of each is best. Our supply is from bottle of Oxygen through regulator and from a 50kg air compressor with an air filter – still looking at the delivery via mask etc – we live ina pretty rural part of Africa and need to set up some system in preparation.
I stumbled on to your article while on a bit of a mission of my own. I thought I might share my idea.
Just a tiny bit of background, I am a retired (to a small town in Italy) aerospace Project Manager/Risk Manager/Flight Test & manufacturing electrician, but my passion has always been motorsports. I’ve built racecars, won races as a driver and owner, etc.…
My idea, and I spent some time two days ago proposing this to the world’s top racing organizations, is to harness the power of these organizations to help with the problems we currently face with our medical manufacturing infrastructure. Nascar, F1, IMSA, FIA, ACI, FIM, WEC, Indycar. So far, no response.
Put the drivers on iRacing, and put the rest to work helping with these problems. Give them season points for production of units.
Carl Haas has the engineering and manufacturing prowess in his groups alone to probably singlehandedly solve these problems. You can add 50 more names to that list. These are organization that are highly flexible and you will find no group of professionals, and amateurs, that can be more single-mindedly focused on a problem or goal than racers.
Just think if your grandpa could have a ventilator designed and built by Mercedes F1. Anyway the PR and marketing opportunities for these organization are endless, but that is beside the point. I see no downside.
If necessary I may see if it would be feasible to take this grass-roots. For every one person working in professional motorsports there are 1000 or more doing these things for fun with similar skills and attitude.
Meanwhile, I’m going to be looking at the technical requirements for a ventilator, how difficult can it be.
If you could help get the word out, or if can help with this issue some other way please let me know.
Let’s kick this things ass!
Best Regards,
Daniel Curtis
Have you guys seen this one?
https://www.geeky-gadgets.com/open-source-ventilator-18-03-2020/
We have a machine shop and specialize in Inhalation Toxicology Instrumentation, company name In-Tox Products…Please provide technical drawings of the Venturi Valve (we have a similar Venturi device) that we can manufacture in a large quantity. We don’t have a 3d printer but this item can be easily machined if we can get the exact measurements including the ID’s and OD’s!
Use of one ventilator for 4 or 8 patients based on previously published feasibility study…
https://www.youtube.com/watch?v=uClq978oohY&feature=youtu.be
I would of thought a ventilator in its simplest form would be a large bellows that acts to apply forced air in, and extract air from the lungs. The bellows would be connected to a Linear Actuator that opens and closes the bellows. The Linear Actuator would be controlled using an Arduino controller to adjust for the correct amount of volume depending on the size of the person. This could be done via a simple potentiometer dial that connects to the arduino that controls the actuator. A second dial could be used to control speed also. This device would not account for humidity. any oxygen tank mixture would be taken care of before the mixture reaches the bellows.
The linear actuator would be a feedback linear actuator as in this link: https://www.firgelliauto.com/collections/bullet-actuators
the Arduino would be from here: https://www.firgelliauto.com/collections/arduino
Don’t reinvent the wheel! What’s needed is an open source 3D printable version of the old Bird Model 8, or even the Army Emergency Respirator (invented in 1965)
Here is a professional reference design for a ventilator, this is serious stuff, not a lot of room for “hacking”: https://www.nxp.com/docs/en/application-note/DRM127.pdf
I found this project on GitHub: https://github.com/covid-response-projects/covid-respirator
How about using microwave radiation at the resonant frequency of the coronavirus particle to break the virus envelop? If we could scale up this process, we could decontaminate N-95 masks so they can be reused. See the following paper: https://www.nature.com/articles/srep18030
Hola Amigos, saludos desde Chile.
Soy Ingeniero en Automatizacion y Robotica (un MAKER)
Veo que aqui mucha gente habla y nada se hace en concreto, yo por mi parte trabajo en el desarrollo de una version VETA open source, tomando como guia las especificaciones del siguiente link…
http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1728-59172011000200006
me pueden contactar al controlyautomata@gmail.com
A few ideas based on reading through the comments from an experienced mechatronics engineer:
– The device should be designed with commodity off-the-shelf parts and 3D printed parts. We’re looking for a single design that is simple to disseminate to the fabricators, and simple to assemble. Take advantage of suppliers like McMaster-Carr who have substantial inventory and can ship 1-2 days in the US. I assume similar parts would be available in other countries. MC can provide the quantity of parts in stock so suggest contacting them for this info before incorporating the part.
– The purpose of 3D printed parts is that if they are designed for DIY PLA printers, then a large portion of the 1,000s of printers in the U.S. can be mobilized quickly to print and ship parts to where needed. Its trivial for anyone with a printer to start printing and most would be excited to contribute.
– For exhaled gas sterilization I propose a circuitous path baffle inside a substantially flat box with an internal UV bulb. The internal baffle parts are laser cut from thin clear acrylic sheet and fastened inside a box consisting of laser cut opaque (UV blocking) acrylic sheet. Again the laser cutters in the U.S. can be mobilized. 3D printed parts can hold the clear acrylic baffle parts inside the box and the outer box parts can be fastened with tape. The air passage would have to be long enough to allow for sufficient exposure to the UV, and with minimal restriction.
– Use of a commodity fan, I like the idea of a PC or server fan that is in stock in high volume and can be readily sourced.
– A sealing face mask can be 3D printed, one for each patient, and disposed of after use.
Lastly, the outpouring of creativity and enthusiasm in this comment section is truly inspiring. And the few comments discouraging the development of this device are truly baffling. Its been stated already, this device is a last resort after all of the existing ventilators are in use. Lets hope we don’t get there.
Could one stop a Aerosolized virus by super heating all air returning from the patient