
Treating the most serious cases of COVID-19 calls for the use of ventilators. We’ve all heard this, and also that there is a shortage of these devices. But there is not one single type of ventilator, and that type of machine is not the only option when it comes to assisted breathing being used in treatment. Information is power and having better grasp on this topic will help us all better understand the situation.
We recently wrote about a Facebook group focused on open source ventilators and other technology that could assist in the COVID-19 pandemic. There was an outpouring of support, and while the community is great when it comes to building things, it’s clear we all need more information about the problems doctors are currently dealing with, and how existing equipment was designed to address them.
It’s a long and complicated topic, though, so go get what’s left of your quarantine snacks and let’s dig in.
As we dig in, let’s address one common point of confusion in terminology: respirators are masks designed to protect the wearer, like keeping health workers from inhaling particles carrying Coronavirus, while ventilators are devices used by patients to help them breathe adequately.
How Our Lungs Work
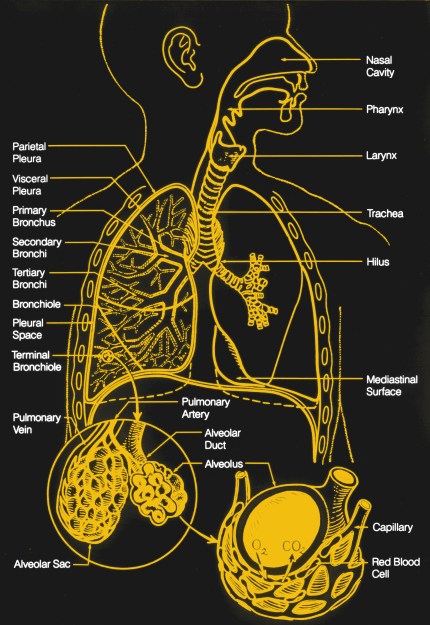
Our respiratory system does two things; it brings oxygen into the body, and it expels carbon dioxide from the body. It does this by taking air from atmosphere and passing it through smaller and smaller structures in the lungs, terminating in capillaries; these are tiny ‘veins’ that are able to pass individual molecules into and out of the blood stream.
The simplest way to imagine this respiratory system is as an inverted tree: a large trunk (the trachea) branches over and over again (bronchioles), ending in tiny leaves (alveoli) that perform the gas transfer. The alveoli are tiny structures like clusters of grapes and are covered in capillaries. The capillaries diffuse molecules of O2 into the bloodstream where they are carried around by blood cells, and take CO2 out. This mechanism is driven by pressure differences between the concentrations of O2 and CO2 in the blood cells compared to the air. The important part is surface area, as the more capillary surface area available to effect gas transfer, the better, which is why the lungs are a lot of tiny spheres instead of two giant cavities.
The gas transfer is assisted by respiration (breathing in and out). The body needs to constantly expel the carbon dioxide-rich air and bring in fresh oxygen-rich air, and this is done by changing the volume of the lungs. The diaphragm (underneath the lungs) and intercostal muscles (between the ribs) both perform work to expand the lungs. This increases the volume of the lungs and air rushes in to fill that volume in each of the small alveoli. Expiration is a mostly passive process; the muscles relax and return to their natural state, much like a stretched rubber band returning to its natural state. Active expiration requires effort from additional muscles.
There are little hairs called cilia and mucus-producing cells throughout the inside of this system. Their job is to capture waste and foreign particles that have been inhaled, and push them up and out, where they cross into the esophagus and the digestive system.
There are lots of things that can cause problems with this delicate system. If the branches are blocked, say with too much mucus, then there’s less surface area available for the gas transfer, and the person can’t get enough air with the same amount of breathing. If the bronchioles or capillaries become stiff (e.g. from smoking) or scarred, then it becomes difficult to squeeze the air out. If the lungs become damaged the alveoli can break down and the lung surface area is reduced, so diffusion is impaired. If the lungs become inflamed the airway is constricted and it becomes difficult to pass a large enough volume of air into and out of the lungs for gas transfer. If the person breathes too fast and moves a lot of air, or too slow and doesn’t move enough air, then their blood gas concentrations get out of whack. Too much carbon dioxide in the blood and the body becomes acidic, which is a problem that other organs then have to solve.
There are other problems that can happen in this system, such as the brain not getting the right signals about the amount of carbon dioxide and oxygen in the blood, or the brain being forgetful about telling the body to breathe. Those aren’t what’s happening with COVID-19.
Why Breathing Becomes a Problem
The CDC has a good guide on clinical management of patients that gives the stats on how the disease presents and what kinds of care they need. In patients that experience the worst symptoms of COVID-19, the problems are pneumonia (infection that leads to the lungs filling with fluid), dyspnea (difficult or labored breathing), and acute respiratory distress syndrome (ARDS). In simple terms, the patients can’t breathe well enough.
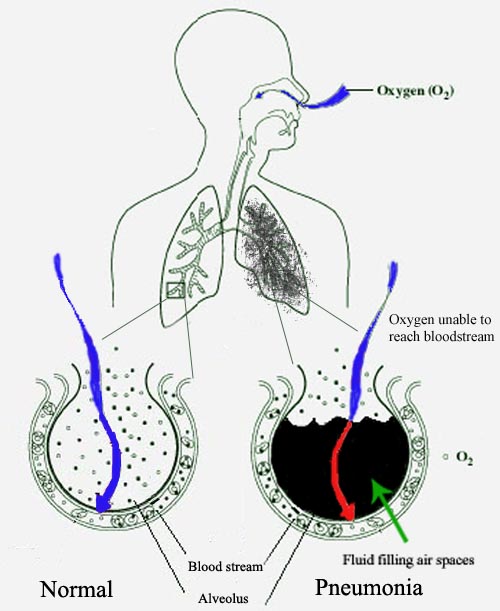
The patient is struggling to breathe because the pneumonia is causing excess mucus production and cell infection, filling the alveoli and blocking the branches and reducing the surface area available for gas transfer. The alveoli that are accessible still work, but there aren’t enough of them available to sustain the patient. The result is labored breathing and insufficient gas transfer, which can lead to death.
According to the WHO, approximately 14% of the infected require hospitalization and oxygen support, and 5% require ICU admission. Looking at Bergamo, Italy, that 14% of the entire population is overwhelming hospitals, while in places that are better prepared, or where the curve is flattened, the health care system is stressed less.
The doctors in Italy are suggesting that the hospitals are becoming epicenters for virus transmission, and that home care may be preferred if possible, especially since they don’t have all of the resources they need. This is what’s causing the DIY community to look at ways to quickly develop some of those resources.
How We Provide Assisted Breathing
There are three main ways to help people who have difficulty getting O2 into their blood and CO2 out:
- Open up their airway to increase surface area
- Increase the oxygen content of the air
- Make it easier for them to breath in large volumes of air
Since air is 78% nitrogen, 1% argon, and 21% oxygen (with traces of other gases), there’s a lot of room for improvement in gas transfer by increasing the percentage of oxygen. Carbon dioxide diffuses a lot more easily than oxygen, so USUALLY it’s not a problem to get the CO2 out. At home this is done with an oxygen concentrator or delivered tanks. In a hospital this is done with central O2.
Another thing to do is to open up more of those passages and clear up the blockages and get at all those alveoli. One way to do that is the same way that works for sleep apnea; positive air pressure. By putting positive air pressure in all the branches, it helps keep those airways open just like gently blowing up a balloon keeps it from collapsing. The only thing is that the “balloon” we’re talking about here is made of delicate tissue that’s already stressed, and over-pressurizing is catastrophic.
We also help get more gas transfer to happen in the alveoli that are still accessible. This can be done by assisting the patient with the effort of inhaling, again with positive air pressure. In patients, labored breathing means they get exhausted just trying to get enough air, so assistance with the inhalation is necessary and this is often where ventilators become part of treatment.
The ultimate goal with these three things is to give the patient time to develop antibodies and fight the virus and clear out the lungs, so the patient could be on mechanical assistance for up to two weeks.
The Ventilator
The ventilator can help with these things. It doesn’t produce oxygen, but passes provided oxygen through it and to the patient. There are multiple kinds depending on the severity of the infection. Ideally you want NIV, or non-invasive ventilation which uses an external mask. Invasive ventilation requires a tracheostomy or endotracheal tube inserted in the nose or mouth down into the lungs, which is an incredibly difficult and risky process that can only be done by a qualified physician in a medical care setting and can lead to other complications.
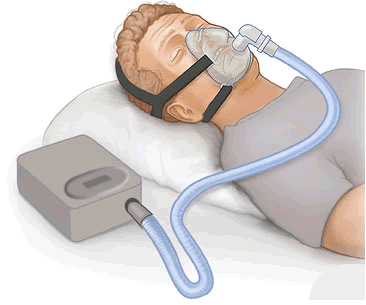
To best explain a ventilator, let’s start with a CPAP and work our way up. Short for Continuous Positive Airway Pressure, a CPAP takes normal air and compresses it and presents that higher pressure air through a hose to a mask. Usually the pressure is between 4-20cm H2O. If you’ve never used one, think about what it would be like to grow up in a swimming pool with your head above water, where your lungs are constantly pushing the water out of the way to breathe, and then after years you get out of the pool. Your muscles have to do a lot less work to bring in the air, and it rushes in easily. The CPAP is the same concept; by supplying higher pressure air, your lungs work less to inspire than they would otherwise and they can take deeper fuller breaths. More importantly, the pressure keeps the passageways from collapsing. Exhaling is a little more difficult, but remember that this is a mostly passive process; the natural elasticity of the lungs and muscles can overcome the increased pressure, within limits of course.
The BiPAP is the next level up. With some fancy sensing, it’s possible to detect the exhalation beginning, and then drop the pressure level down for the exhalation, making it easier to breathe out. You’ll see an IPAP and an EPAP number, which is the inhalation pressure, and exhalation pressure. Note that in both cases it’s still positive air pressure; we can’t have the passages collapsing on exhalation either. The other advantage is that with a greater difference in pressures, you can have a greater tidal volume (the amount of air that goes in and out in each breath, typically about 500mL or 7mL/kg of body mass) because the greater IPAP allows for more in, and the lower EPAP allows for easier expiration.
The ventilator is the next logical step. It can adjust the pressure either reactively or proactively, or both with special limits. For example, it could allow the patient to breathe on their own with BiPAP-like support, but ensures that the patient is breathing at least a certain number of breaths per minute, or it could take over the breathing process entirely and increase and decrease pressure at specific times to make the patient breathe when they couldn’t otherwise on their own.
Some ventilators are designed for home use, where the system vents the expired air directly from the patient, and the patient is relatively stable. With these ventilators the tube can be connected to a mask or to a tracheostomy tube.
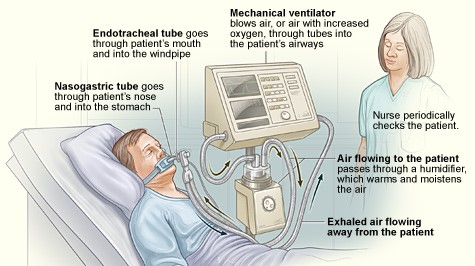
Other ventilators are designed for acute hospital use. These have much more complex interfaces for the variety of treatment modes for which they are capable. They typically do invasive ventilation in which an endotracheal tube is inserted in the nose or mouth and down into the lungs. The biggest factor here is that the expired air is captured by the system and filtered before being released. In an application where the patient has a transmissible disease, this point is particularly important.
Most of these machines have an additional port that takes in supplied oxygen. This can be tanks, but not likely because of the high rate of flow needed. An oxygen concentrator can only supply about 10L/min. In the case of acute hospital ventilators, much more may be required. Most hospitals have central O2, capable of supplying up to 50L/min.
The Many Challenges of Ventilator Design
Now that you have the basics behind the tech, here are some specific challenges.
- You must have a good seal on the mask the person is wearing on their face. If you don’t have a good seal, the mask will leak and you won’t be able to maintain positive pressure. Poor sealing is one of the main reasons for these kinds of devices to fail.
- Monitoring expiration is important. The face mask must allow expired gases to leave, or else the patient will be rebreathing their own air. The machine knows how much it vents and takes that into account when supplying pressure. When the patient breathes out, the expired air doesn’t go into the machine, it goes out through the face mask vents and into the air. In a hospital environment, this would be aerosolizing the virus, which would be very bad, which is why the there are ventilator designs for hospitals that capture the expired air through a different tube and filter it.
- You have to maintain the level of positive pressure consistently; if there’s a leak you have to ramp up to maintain the pressure level, and if the leak is plugged you have to drop down immediately. If you go above the pressure level intended, you can easily do damage to the lungs. Pressures are typically in the 4-40cm H2O range. This is a big important requirement, because messing this one up does a lot of damage fast.
- You have to heat and humidify the air. Usually the sinuses do a good job of this, but on a ventilator, this isn’t possible because the sinuses may be bypassed. When the air is too dry, it can lead to hypothermia, bronchospasm, extra mucus production (which is bad because it blocks more passages), or other problems.
- With warm wet environments comes bacteria growth, and Legionnaires’ disease, a severe form of pneumonia caused by bacteria, is a serious risk in already compromised patients. Having an unsanitary environment could quickly cause problems worse than the original disease.
- You have to be able to supply a lot of oxygen. A portable oxygen concentrator (POC) won’t work for a couple reasons; First, it doesn’t pull out enough oxygen for the patients that have needed supplemental O2 so far. Second, it only dispenses oxygen when it detects breath, but since there’s positive air pressure going in, the sensors on the POC won’t work. Depending on the needs of the patient, a larger oxygen concentrator might be sufficient, but any ventilator design needs to allow for an oxygen inlet.
- The good news is that you only have to be able to supply positive pressure; ventilators do not suck the air out of the lungs. They merely provide varying levels of positive pressure and let the elasticity of the ribs and diaphragm take care of the exhalation.
- Either you’ll need lots of sensors (PaCO2, TcCO2, SpO2, FiO2 in addition to flow and pressure) and the ability to have complex algorithms, or you’ll need an expert constantly monitoring the patient. If they roll over and pinch the tube, or move and break the seal, or get agitated, or their condition changes in any way, it may be necessary to change the settings of the machine. The software that runs on existing devices is complicated, with good reason. You may not think about your breath rate throughout the day, but your body is regularly adjusting the amount of air it needs, and the system has to account for that.
- An adult male lung has a volume of about 5L, but tidal volume is roughly 500mL. This means that the system needs to be able to supply pressured air for at least 500mL per inhalation, and may need to keep applying pressure for the exhalation.
- Any design needs to be manufacturable using existing parts that are readily available. The reason for the shortage of ventilators now is that demand jumped faster than the manufacturers’ abilities to create product. They already have supply chains, manufacturing lines, injection molds, and working designs that are tested and proven. The only thing holding them back is their ability to source and assemble the components fast enough, and then distribute them, and you better believe they’re throwing every resource they can, with the assistance of every government, at solving all of the supply chain problems they have now. The entire point of flattening the curve is to give everyone as much time as possible to solve problems.
Using Ventilators Requires Highly-Skilled Health Care Workers
Besides the physical constraints of a machine, you need trained physicians to monitor the patients. IF you could get a DIY solution, these are the other things to consider.
- Each patient will need to be titrated and adjusted regularly. This is the process of figuring out what the right levels are for giving the patient treatment. There are multiple variables, like the inhalation pressure and exhalation pressure, whether the machine is leading the breathing cycle or the human, the rate, the sensitivity of the sensors. There is a huge risk of damaging the patient’s lungs through negligence. If the settings aren’t exactly right, then the patient could end up having to do more work fighting the machine than they would be doing without the machine, or have an improper blood gas balance. For example, if the EPAP setting is too high, the patient may be taking in more than they are exhaling, which is clearly not a sustainable solution.
- The same goes for O2 levels in the supplied gas. Since increasing the O2 levels can lead to flammable or explosive situations, it’s important that the system not leak and that there are sensors and protections in place to ensure that the O2 is going to the right place in the right amounts. Also, supplying too much oxygen can suppress the brain’s “drive to breathe” mechanism, the signal telling the respiratory system to breathe in and out, leading them to stop breathing.
- Cleanliness is essential, as it could cause issues worse than the original disease, and the ability to keep the machine clean even if it’s only used for a week, is critical.
- In most cases where a ventilator is needed, the patient has comorbidities (additional medical conditions) such as hypertension, diabetes, cardiovascular disease, and respiratory system disease (also here), which makes treatment more challenging.
- The biggest thing is that if the person’s conditions are so severe that they’re on a ventilator, then they’re going to need to be near immediate care, which means the solution has to be in a hospital setting. Even if we had a surplus of ventilators, the number of ICU beds and critical care staff would end up being the limiting factor.
- Any new device will require training of the caregiver, so it needs to work like existing units with which they are familiar, or be really easy to learn.
- It needs to be said that proper resource allocation is important here. We can’t have anyone hoarding ventilators for anticipated need while people are dying without them. Every ventilator that comes off a production line needs to go to a patient in need, and we should move them around as we can.
Current Manufacturing Efforts
The companies that make the necessary machinery are well aware of the problem and are ramping up production as quickly as they can. In addition to increasing production of the right kinds of ventilators, they are looking at CPAP and BiPAPs and non-life-support ventilators and exploring ways to take these medical devices with all of the appropriate safety mechanisms and certifications already in place and production lines already set up, and trying to find ways to adapt them to the specific needs for COVID-19.
One of their biggest problems right now is supply chain. China was shut down for a long time. Transportation routes are in disarray with airlines having fewer flights, countries closing borders, and even in the best of times shipping by sea takes a month. I know that GE has opened job postings for laborers to work on their assembly line in Madison, WI where I am writing this article, and I assume others all over the world are ramping up production to the best of their ability. Shifts are getting added, processes paralellized where possible, and injection molds warmed up. Setting up additional manufacturing lines might help, but it takes time to make all of the specialized equipment necessary. Even if new factories could retool quickly, the routing of components may be the more limiting factor and it’s quite possible that a specialized component will be a limiting factor for the entire industry. If production depends on a specific part, and an assembly line is already consuming that part as fast as it can be made, adding a second assembly line doesn’t “make the baby” any faster.
Some are looking into creative ways of multiplexing existing ventilators, just last week we saw Dr. Charlene Babcock demonstrate one way to convert a single ventilator for use with four patients based on a n emergency medicine feasibility study. As an exercise, try syncing your breath with someone near you and maintaining it. Even if you can get it to work for an extended period of time, you’d have to take into consideration that in a hospital all patients would have to be on all the same settings, with synchronized breaths of the same volume, they would all have to have the same resistance, and any change to any of them might mean that patient was no longer compatible with the other patients on the ventilator. Basically, it only works if you make them unconscious, and even then only briefly.
Conclusions
The DIY community is fantastic, and has a lot of bright people who are very capable of a variety of things. We’ve already seen 3D printed parts come to the rescue. Personal Protective Equipment (PPE) is being hacked together in rapid order by hackerspaces and 3D printing companies. Ventilators, though, are a whole new beast with a complexity similar to life support in a spaceship, though different enough that asking a car company to make one is like asking a ventilator company to retool to make a car. Asking a car company to make PARTS to help with supply chain problems makes sense, though. See the requirements put out by the UK for a ventilator solution for a more thorough guide to what’s needed.
My hope isn’t to discourage entirely; my hope is that this 101 will help guide a little so that effort isn’t wasted on solutions that can’t work. There’s an argument that “if there aren’t enough ventilators and patients are being turned away, I’d rather have a slim chance with a hacked solution than no chance with no solution. The reality is closer to “if there aren’t enough ventilators, a hacked solution will most likely do more damage than good, take up too much time from already strained health care resources, and could lead to death.” As the Hackaday community isn’t one for shying from a challenge, though, if you’re going to start somewhere, you should start with existing solutions that are close and in no short supply, like oxygen generators and BiPAPs and some kinds of ventilators, and look into how they could be modified without bypassing the safety mechanisms built into them, rather than start from scratch. As a community, we can and should help whenever possible. Let’s do it alongside the guidance of trained health professionals who have the skills to navigate the needs and the risks of assisted breathing.













Somewhere in there is the iron lung for completeness sake.
Bingo! And that’s the thing that everyone’s missing. Some “iron” lungs were made out of plywood. Plywood, a vacuum source (shop vac would do) and a timing controller might get more people by than not–especially in undeveloped world. “But let’s reinvent the wheel”
the Iron lung worked well during the polio epidemic where the disease caused a neuromuscular inability to breathe. Covid-19 causes infiltrates and stiffens the lungs greatly, rendering the negative pressure iron lung type of mechanical ventilation totally ineffective, thus leading to ‘positive pressure’ ventilation.
“rendering the negative pressure iron lung type of mechanical ventilation totally ineffective”
How do you figure that? All “positive” or “negative” pressure means is to have a difference in pressure on the inside and outside. You can move a piston back and forth by either decreasing the pressure on one side or increasing it on the other. The main difference is “how big of a device do you need?” A negative-pressure device needs to be bigger than the person and also prevents access to the person’t body other then via the arm gloves. The person is also more limited in mobility, moving devices in and out of it needs an air-lock, etc. Where-as a positive-pressure ventilator could (in theory) be the side of a thimble as long as you had a power source to move the air in it (of course, with today’s technology, it’d have to be much bigger but the idea is that its minimal size is not limited by the body size.)
Super simple and I guess maybe can use some updates?: https://www.appropedia.org/Negative_pressure_respirator
A couple of other notes that seem to have been overlooked:
1) Oxygen Toxicity – Supplied O2 can lead to increased risk of toxicity:
https://www.medscape.com/answers/304068-104801/what-is-oxygen-toxicity-in-mechanical-ventilation
2) Drive to Breathe – Reduced Drive to Breathe was noted, however this is only a concern with patients on nasal cannulas or various masks. Intubated patients on ventilators can force the patient to breathe.
I was an ICU nurse for over 10 years and drive to breathe was something we talked about in school and not that much in practice.
This was an excellent summary, and I’d add only two points:
1) In high enough concentrations, oxygen is toxic. A complexity not mentioned is that one often is trading off pressures at the edge of doing damage to the lungs with oxygen concentrations that are at the edge of doing different, but equally bad, damage.
2) As KS notes, the ordinary tidal volume of around 8 mL/kg is only about 10% of the full lung volume, but the normally-unused volume can’t be ignored. Even when you are at rest, every minute or so you unconsciously take a much bigger breath, with the effect of opening up some of the airways that aren’t needed for your resting O2 requirements. If you don’t do that, you increase your risk of infection in the inactive alveoli. That is why when you might be content to breathe just enough to oxygenate (if you have broken ribs, or have just had abdominal surgery), nurses will harass you to force you to take deeper breaths now and then. Ventilators have to do that too.
-RRF, MD
I see a lot of people talking about their ventilator projects being asked about things like pressure and volume measurements and other more complex features, and these questions are usually dismissed by pointing out that we’re desperate at the moment.
Do you have any insight about this, Robert? Will simpler ventilator projects not be used even in the crisis? Or do they have a role to play?
Thanks for any info.
Fantastic article, very clear and concise. The instant reaction to such crisis is how can we use our skills to help, unfortunately effort is not enough and can often result in poor use of critical resources. The best thing we can hope for is that supply lines and other resources are streamlined and prioritized for existing manufacturers.
Having been a Registered Respiratory Therapist for the past 28 years, this is not a DIY task. We don’t need to reinvent the wheel here. There are plenty of “old school” pieces of equipment that would fill the void here. The Bird Mark 7 and Puritan Bennette PR 2 are both perfectly capable of delivering Time Cycled, Pressure limited ventilation to a patient. There are other “plastic vents” made for transport that can be mass produced and rapidly deployed that work on the same principles as the afore mentioned machines. The problem is they do not have any kind of alarms or monitoring capabilities. This makes the use of them not possible because a nurse or RT would have to remain at the bedside 24/7. It would be better served if you could DIY something that could be put inline with these devices providing feed back on Rate, Tidal Volume, Minute ventilation, and Peak Pressure. Also provide Alarm Limits for High and Low Pressure, High and Low PEEP, High and Low Rate. With these things being able to monitor and alarm when needed it frees the nurses and RT’s to care for more than one patient at a time as we do with existing ventilators. Just my two cents here, but if you want to help? That’s what we need…….
I do believe the monitors you mentioned shouldn’t be “too tough” to implement to inline with the rest of the unit. By “not too tough” I don’t mean easy. It’ll be a challenge to be sure. But it’s feasible. It can be done. It’ll be a lot of effort, and I think, worth it.
One thing to be aware of is for automated QA: To see that it all works correctly we’d need the base device and something to automate the testing, to ensure the monitors are actually reporting correctly. This is where device testing becomes time consuming, and requires significant attention to detail. (i.e. This raises questions like: Was it the new monitor that misbehaved, or the verification device? How do you make the determination? …etc. )
I agree JD, there are analog devices to check each of these measurements individually. The problem is having a device that can do them all at the same time and provide feed back/alarms that is the difficult part.
Just checked Ebay with limited success for either unit. Does anyone have suggestions on where we might source a few devices for testing, and where the wider Hospital community might source more for implementation (assuming a functional device is created)?
to measure tidal volume and minute volume, a Wright Respirometer used to be the gold standard.
there are a few available (https://www.ebay.com/sch/i.html?_from=R40&_trksid=m570.l1313&_nkw=wright+respirometer&_sacat=0) but they are expensive. Pressures may be measured with an analog airway pressure monitor (https://www.ebay.com/itm/LOT-of-17-GAUGES-with-PAW-AIR-PRESSURE-FOR-BREATHING-CIRCUIT-GASES-Pa-X-100-kp/264471355913?hash=item3d93b8a209:g:htQAAOSwuhNdg9JN) or digital transducer measuring up to say 60-70 cmH20 pressure
If one were to add monitoring and alarms to something like this:
https://www.mercurymed.com/product/go2vent-2/
https://youtu.be/X7dxuj81ECs
Would that be a workable replacement in cases where a ventilator is not available?
I believe this could be a chance for the younger people of the world to help out as they are asymptotic. With a short class they could be trained to monitor one or maybe several people at once. Not make medical decisions just verifying equipment is preforming. Similar to candy striper’s in the past. Must relief nurses and doctors to preform the medical care that is needed. The human is the most adaptable control and monitoring system on the planet. The electronic solution may take to long to implement. But it should still strive ahead to relieve the first monitor system as industry gears up. 🙂
Hi Oliver,
Just to be clear, did you mean to say that young people are asymptomatic? If so, I’d like to try to clear up a misunderstanding. While some people, regardless of age, can be asymptomatic, young people have the same chances to develop symptoms as everyone else.
Also, asymptomatic just means “without symptoms”. A person who is asymptomatic can still carry and transmit a virus to another person.
Wishing you the best. :)
“A person who is asymptomatic can still carry and transmit a virus to another person.”
Agreed.
And they would also have to be trained in procedures such as cleanliness, etc that come into play here that even those in the medical field don’t always follow properly (not dis’ing the doctors/nurses in general, mind you. But, as in ANY group, there are some who know what they *should* do but don’t always do it. And someone who hasn’t had it pounded into their head for several years is even more likely to not follow protocol.)
Maybe with a week or so of general training, you could pull in “candy-stripers” but the training would take other people away from their jobs for that period. But giving someone a 30-min talk and then saying “have at it” would not, IMHO, be a good idea. Now if we were able to completely quarantine a full section of the hospital and “no-one leaves without isolated quarantine for 14 additional days” then maybe it’d be workable. Or if it was a disease like Ebola (where the quarantine period would be much shorter. Symptomatic people show obvious symptoms and the disease only take a few days to be symptomatic and is not transmissible until symptomatic) then maybe it’d be workable/worth the time and danger.
This was a very enlightening article, thank you!
As someone who sleeps every night using BiPAP 15-20cm with 2L/min O2, it was fascinating to read about some of the details pertaining not only to my equipment, but also to my lungs and how they function.
Purely mechanical reliable pressure regulation: https://www.youtube.com/watch?v=z985abJITQE
That is amazing. Just needs a float valve (like in the toilet) to account for evaporation of the water. Can’t have nurses running around with watering cans in the IC. ;)
Also, I’m not sure about the temperature of the water. I think it will probably need to be warmed a bit.
That looks like it’s for positive end expiratory pressure, i.e. the air its metering has already left the patient’s lungs.
The temp of the water wouldn’t matter (I don’t think) since it’s the exhaled air, not the inhaled air, that’s making the bubbles.
As to a float, there’s another way around that. If the device itself was attached to a holder that held it in place in the tank, then the level could be adjusted by moving it up or down in the water (rather than moving the water level up and down. The distance from the top of the water to the bottom of the bubbler is what is important.) “But we STILL have the issue of the water evaporating!”, you say? You put the tank into a sink (or even on the ground) with a steady drip of water going into it. Then the tank will overflow any extra water and it will remain constantly full. So no moving parts needed to keep it at the same level (the only moving part in that part of the apparatus is the weight and that ALREADY has to move up and down) and no extra parts needed other than the support for the device (they don’t show how it’s currently held in a vertical position but are hand-holding it in the video but a simple sleeve with a lock-bolt would work and make it adjustable.)
I see a related and potentially significant issue being that of delivering sufficient medical oxygen to facilities with existing supply chains and infrastructure. High flow nasal cannulae need 60 or 70L/min, and routine ventilation might need flow rates up to 10L/minute.
Maybe someone could turn their mind to ways to safely use industrial oxygen equipment, necessary adapters, and how best to filter out impurities from industrial oxygen.
The other issue brought into stark relief by COVID-19 is the safety of the surrounding treatment team with potential aerosol spread from the exhaust circuit, and the need for suitable filtering which must be addressed. Similarly, endotracheal intubation and laryngeal mask insertion are considered procedures with a high risk of aerosol generation that should ideally be done with full PPE in a negative pressure environment and attention to reducing the likelihood of coughing during intubation with suitable induction. Maybe there is scope to improve techniques and hardware to reduce the risk of aerosol dispersion during intubation, perhaps with suction circuits.
The relevant standards will be available for free for this period, an example being here https://www.bsigroup.com/en-GB/topics/novel-coronavirus-covid-19/ventilators/ (the full list is here https://www.cencenelec.eu/News/Press_Releases/Pages/PR-2020-003.aspx )
Great article! Very informative.
One small correction:
“The gas transfer is assisted by respiration (breathing in and out)”
Respiration is actually the chemical reaction, not the act of breathing.
The thing is those with say COPD that are at higher risk of severe complications have different needs. The scar tissue alone causes the body to not be able to remove CO2 as efficiently as a healthy lung. CO2 is a bigger molecule and most copd PT don’t have a issue with getting O2 in. The co2 builds up and makes the blood acidic and that doesn’t feel good.
Practice pursed lip breathing now in case you do happen to catch this. It helps open the air sacs and allows better gas transfer!
Great education for the layman. Thank you.
https://www.ventilaid.org/
Open Source Ventilator Design. Anyone capable, please consider making…
I just skimmed the report. Missing from it might be the reality of ventilator use for Covid-19. The best success rates come when patients are chemically paralyzed, sedated, and prone – face down. Paralyzed so they can’t fight the ventilator, which is not monitoring CO2 and therefore the breath reflex. Sedated to avoid panic over being paralyzed, not able to swallow or cough, etc. Imagine a couple days of continuous waterboarding.
I can’t see this as a DIY situation. Iron Lung type breathing assistance, perhaps. PP ventilation, not so much.
Another guy on the right track, negative pressure ventilation supposedly works for ARDS. Plywood Iron lung time, everybody. Seriously, it’s simple!
YES< YES< YES!!!
I was a rural western US flight and fire/EMS paramedic , also a paramedic instructor, many hours minding vented patients on long rural to urban transports; we were about to get a pneumatic vent when I had to take a medical retirement. I also designed the functional 3D printed SCUBA regulator edu-demo which was featured on Thingiverse a few years ago.
DIY is not what we need, likely something long tested that can be engineer adapted easily to mostly mass injection molding with a few brass valves. I have not had the opportunity to tear down a vent but I assume that the best all pneumatic ones are pretty simple inside with most adjustment being valve spring pressure.
Robot hands gripping BVM are also not on target, nor are DIY crappy 3D printed kludges.
We can also plan to make these disposable and cut durability corners to get them delivered quickly.
If we are stuck as far behind the 8 ball as DIY kludging vents I think either hand bagging or iron lung are the only realistic ways to go for respiratory support even with the limitations.
It is more important to pick a design or several which are easy to produce quickly and get them in production by the end of the week, we are already way behind the power curve.
More difficult we also need a crash RT-lite training program, probably grab every experienced diver as they have already tested competence in understanding basic respiratory A&P and they are mostly not already first responders or hospital caregivers; a pool of people ready to be shotgun trained to provide basic respiratory therapy in mass ICUs working under the supervision of experienced professionals.
in response to glvrrt
A few more points, regarding issue 2.
We derive our drive to breath from our bloods pH, slow breathing → build up of CO2 (as article points out easy to blow off CO2) → pH ↓ → increase breathing.
It is sometimes hypothesised that people with emphasema/COPD derive their drive to breath from hypoxia (low o2) but as far as I know this has never been shown to be the case and it’s likely that changes in the blood and air supply in the lungs (V/Q mismatch) explains their seeming reduced breathing drive on high flow O2.
As you point out it’s moot as the ventilator should have a madatory rate and pulse oximetry (which is dirt cheap and simpler to make). So it can flag falling sats and changes in respiration rate.
Finally **most** of managing a ventilator is pattern recognition. Stuff that you can easily turn into an algorithim so long as you can get an idea of lung compliance (montiroing pressure as volume changes).
If you don’t want an AI running the show you can just show the values to an aesthatist one after another. Ditto for blood gases and they can easily decide the next change to make.
There is a process of direct oxygenation of the blood but this is still very experimental. The blood can be oxygenated but it is the removal of carbon dioxide which is difficult. Some experiments in rabbits turned blood into carbolic acid. If this could be managed and successfully keep up with the human lung size the gains would even overcome complete lung failure and blockages.
Isn’t that called a heart/lung machine? (Granted, there’s probably only enough of those to handle a small percentage of the patients who need it…)
I’ve been thinking about the task on enriching the air, much less the complex delivery system via a ventilator, and specifically thinking about the simplicity of a tent, fan and O2 generator.
For if oxygen support is provided on some graded scale, from no support at all, through some ambient enrichment, through delivered enrichment, right up to fully assisted breathing, surely there must be some value in the DIY community attending the lower end of that scale, rather than going all out for the complexity of a ventilator.
Indeed, easing someone’s breathing this way at home might remove the need for a ventilator or bottle supplied O2, and thereby reduce the need for more advanced devices, and prove useful when no other options are available, where breathing has become laboured, but is not yet critical. Only slight oxygen starvation last year sent someone I love into a full on panic attack and resulted in an ambulance call. So if an elderly person here was struggling to breathe, it would be good to know that something DIY could be assembled easily from common things that could make an immeidate and positive difference.
How hard would it be to create a make-shift polythene tent, and simply add greater oxygenation to the ambient tent air, using perhaps some server fans, extractor fan ducting, a PSU, and a plastic electrolysis bucket with suitable hoses for introducing the O2 to the tent, and venting the tent to an open window?
I know this is not a ventilator, I just think it’s a bit late for coding software as a solution in time to offer help.
I think with electrolysis you can by far not generate enough oxygen without overloading the electric grid. An oxygen concentrator is much more energy efficient and is considered by some people also to deliver not enough O2. There were numbers up to 50 or 60l/min.
That’s about 2,5 mole/min of O2, equal to 10 mole/min of electrons
Unfortunately the faraday constant (Ampere-seconds per mole) is quite high, nearly 10^5 so you need about 1MAs/min or 16kA of current at a voltage for sure higher than 1V, lets say 2V. Therefore you need ~30kW_el for one patient and 15kW of waste heat You have to cool that electrolyser like crazy.
Even if you can reduce the amount of O2 by a factor of 10 (5-6l/min) this remains 3kW.
And probably you can not use the generated H2 on site, so most of the energy is wasted.
I think the only applications where breathable O2 is generated by electrolysis are:
1) nuclear submarines under water
2) space applications like the ISS.
In 1 they have plenty of power and cooling water surrounding them and this way they are independent of external supplies.
For 2 it’s easier to ship water to the ISS and store it there for prolonged time than O2. And they have a constant supply of solar power (no clouds in space). The waste H2 is vented and does not contribute too much to weight of the H2O. And they are only a few people in the ISS.
But for a greater number of people on earth I can’t see this as an option.
It is called an oxygen tent and used to be the standard way to administer long term oxygen in hospitals or at home. Used for everything from post heat attack recovery to emphysema. If this becomes a common DIY solution, beware. Humans burn like crazy in in high oxygen environments. Especially fat ones.
The reason you see “No smoking. Oxygen in use” is not so much the fire hazard (when you’re talking about someone at home) but because if someone’s on oxygen, the *last* thing they need is second-hand smoke. Now in hospitals or in an industrial setting, you may have *other* gases/substances that are flammable and thus a higher risk. But in a home setting, a DIY oxygen tent probably wouldn’t have all that much of a super-enriched atmosphere.
Couldn’t sanitizing the exhaled air be easily done by passing it through an electric arc (UV + ozone) and then discharging it outdoors?
Only saw a passing mention of the iron lung a one in first reply. This is only an article about positive pressure ventilation. I would like to see a comparison to negative pressure ventilation, not to replace what is being used but to open a new avenue which already has a widespread and diverse but very large local capability in production by small facilities.
Fra just cleared alternativeshttps://profreg.medscape.com/px/sso/oauthlogin?oauth=1&client_id=29210617-47A2-49CB-A6C8-38A252ED3F14&response_type=code&redirect_uri=https%3A//www.mdedge.com/services/medauth/authenticated&state=https%253A%252F%252Fwww.mdedge.com%252Finfectiousdisease%252Farticle%252F219591%252Fcoronavirus-updates%252Ffda-allow-alternative-respiratory-devices-treat&status=5e7beaa574c9b
(My replies do not seem to thread)
re:Alex Rossi
Pulseox is a VERY unreliable indicator, people can keep a very good o2 sat while their blood acidity gets to the point where thy are left with a pickled dead brain and only an agonal brainstem. Capnometry(end tidal CO2) sensor on the ET tube is where the real information comes in for intubated patients. I think it is an electronic acidity sensor(h2o+co2=carbonic acid). The capnometry sensor curving with the vent also gives good proof that your ET tube is still in place.
I’ve joined a few projects and gave advice on how to make the electronics safer to use. The general electronics skill level is very poor. I’ve attempted to teach them from my years of electronics experience and add the basics on electronics safety guidelines*. After a few attempts one group member got angry with me for ‘spreading misinformation’ and told me: “Mechanical respirators are not that complicated. It’s not rocket science.”
In the future I would like to do a talk on ‘electronics design is harder than you think.’ To inform not to discourage.
*Note: the safety guidelines are not representative of the medical guidelines. I do not know the medical electronics guidelines and can’t teach it.
Check this> https://www.ventilaid.org/
1USD bottle here:
https://www.bbc.com/news/business-40498395
The entire world talking about ventilators reminds me of a really bad joke: “Two engineer neighbors are standing on their respective back porches, talking about a lost antique pocket watch that the kids hid and lost when playing pirates and treasure chests. The bereaved engineer says, ‘I’m optimistic I can optimize this porch light to search my patio more thoroughly.’ The other neighbor, looking at the bereaved engineer standing on clean, and empty porch, under the porch light says, ‘But the kids were digging in your yard. Why would you look on the porch?’ The bereaved engineer neighbor says, ‘That may be true. But the porch is where the light is!’
The ventilators are about as useful as iron lungs. As a physician, and in the academic emergency medicine world…I know and hear way too many dispatches from “the front lines.” And resoundingly, the problem is ‘ground glass appearance’ on CT’s and X-rays of patients’ lungs. That picture description is from the fibrosing pneumonia overwhelming their respiratory system.
For context of the lack of functionality this is causing, imagine a scab covering almost your entire skin from the worst scraping of your skin imaginable. Now, take that completely scabbed-over person and put them in a sauna. They simply won’t be able to regulate their temperature by sweating. The resulting hyperthermia will cook the scabbed-over person from the inside out.
See, its the fibrosing that is killing the patients. The ventilators are trying to eek out every possible bit of O2 and CO2 exchange from what little functional lung tissue is NOT YET FIBROSED (and this is a progressive pathophysiology).
So what am I saying? If you guys can be genius in the gears and nuts and bolts and software- we need to have a discussion on making exterior lung assistive devices. We need to make a gaseous exchange interface that we can run blood through. THIS is what we need to change the mortality rate.
The ventilator is the light we have…and we don’t even have enough of them. But the ventilator is only an assistive device in overcoming this disease.
Medically speaking, we need to take the lungs offline, flush them, and then optimize the surfactant barrier. The body does not have an effective way of removing malfunctioning fibrotic processes. And this virus is killing all of us from THAT biological defect.
Like peritoneal lavage using perfluorocarbon fluids. Still going to need some pumps and tubes. Get on it Doc. Let us know about the tubes and pumps you need.
I think the idea of this blog is crowd sourcing ideas you never know where they will come from or go to. People here are trying to find ways that we can get as many people involved at all levels of skill and means to throw at the problem not as a silver bullet but, as an unstoppable force. I look at it like habitat for humanity. Contractors are brought in to oversee a bunch of people with, little or no skill ,to o construct a house. They use very little of modern tech like nail guns and compressors. They put the stuff we have a lot of to work (muscle). If you want to tear down the side of a granite mountain, you can use dynamite or a bunch of men with picks and shovels and. Someone to show the way. If you are out of dynamite you don’t just stop. You can even do both in tandom to an even better outcome.
Sorry to sound snarky. Thanks for the heads up. I’m off to talk to some people about gas exchange.
You can’t use both dynamite and men with picks in the same area but yes, in some cases, using them in separate areas works.
But the analogy does fail in one respect: You’re not going to have much effect on granite with a pick. “With a sledge-hammer?” yes. “With a drill and an absorbent wick material and some water?” Maybe. “With a pick?” You may make a few chips fly but you’re going to blunt the pick *long* before you do anything with the rock.
– As i understand the whole exchange in alveoli takes place between water and air, water and red cells. Not directly between red cells and air. We have great ways to saturate water with oxygen, to remove dioxide from water. I understand there are issues in-between, but don’t we have solutions for all of them?
– I remember a small percentage (1-2%) of respiration (cutaneous) takes place through skin (In bats this is up to 12%, making them more tolerable to respiratory hazards). Doesn’t that mean that the patients would better have their skin more exposed and aerated? Wouldn’t there a high positive pressure increase this exchange? 1-2% is not much, but maybe it gets 4% with doubling the pressure? When you are left with 30%, 4% is something.
Here is an article detailing ECMO: The Potential Role of Extracorporeal Membrane Oxygenation
https://jamanetwork.com/journals/jama/article-abstract/2761778
Very interesting note. I can see they are portable also, less than 10kg! It seems that hundreds of ECMOs have already been ordered around the globe, by the major countries at least.
the survival rate of ECMO is zero 0.00%.
If you are to the point of ecmo, you are probably beyond recovery. Got to get ahead of that point.
Since the sars cov2 virus has an outer coat that is easily damaged by alcohol and young people have been vaporizing and inhaling ethanol recreationaly, would it be possible to beliver a dosage of vaporized ethanol to the lungs that is large enough to damage the virus shell but low enough to avoid damage to the patient?
Could this be used as a prophylactic or in early onset of the infection before the lungs have sustained damage?
Could ethanol vapor be used with surfactants?
This is the wrong forum for this dscussion, but I couldn’t find a better one. If anyone knows a better place to post this, let me know.
Since it seems u r interested, ncbi (ncbi.nlm.nih.gov) has a lot of scientific articles on the issue. Also,a very informative NHS page lies here: https://www.gosh.nhs.uk/conditions-and-treatments/procedures-and-treatments/extracorporeal-membrane-oxygenation-ecmo
If you are on ecmo, your lungs are probably beyond repair. This is the wrong place to post this but I couldn’t find a better placeSince the sars cov2 virus has an outer coat that is easily damaged by alcohol and young people have been vaporizing and inhaling ethanol recreationaly, would it be possible to beliver a dosage of vaporized ethanol to the lungs that is large enough to damage the virus shell but low enough to avoid damage to the patient?
Could this be used as a prophylactic or in early onset of the infection before the lungs have sustained damage?
Could ethanol vapor be used with surfactants?
If someone knows a better place to post this, let me know or pass it on. Thanks and good luck
I have been pondering what you said up there, doing some reading, and have decided I’m taking a package of baking soda with me if I have to go into hospital with this, with instructions to flush my lungs out with a mild solution of it if it gets real bad…. works great on my sinuses.
For cilia in the lungs that no longer move to help clear the junk out of the lungs there’s a very inexpensive device ( $20 or so if I remember correctly) that when blown into will send a sonic wave down into the lungs to break the stuff loose. There is also a device that is worn like a backpack that will move the diaphragm to act like a ventilator of sorts . I have no medical training so forgive me if I am over simplifying things.
My device is a “Community Ventilator”, not individual units. It would supply low pressure air with a small steam injector for humidity, temperature control, oxygen enrichment and valving that can vary in size and rate. Recovery of the expelled vapor/air is negative pressure from the incoming side of a power burner and incenerator fire box. ALL of the expelled air is put into the burner, There is no “filter” that later has to be handled or disposed of….the virus is toasted. One 20′ container would service about 100 patients
All these 100 patients would need to have similar characteristics though (lung volume, etc) otherwise you need to adjust the stream for each patient individually down the chain.
The source of air would be continuous (low pressure) and getting rid of the expelled air would be too, but 2 separate systems. A rotary valve could be used at each patient with size (of the air inlet) and exhaust and speed controlled…so yes, there would be individual control, just not individual source of air. Most important is the exhaled air going to an incinerator, never going back into the system. Exhale would be a reed valve (low pressure check), right in the mask
Calling All Firmware Hackers: Firmware can change common home CPAP machine into ventilator.
The ResMed AirSense 10 is one of the most popular bi-level home CPAP machines. ResMed also make a ventilators. Their ResMed AirCurve 10 is identical in tems of hardware. It is firmware that limits the AirSense blower to 20 cm/h2o and limits the EPAP range. This ventilator firmware also the ASV algorithm to constantly learn the patient’s unique respiratory rate and deliver pressure matched to patients’ breathing, adapting dynamically to their changing needs.
If someone here can dump the V19 firmware from a ResMed AirCurve, and show us how to flash an AirSense, the world will have millions of emergency ventilators available.
My country has 30 ventilators, and hundreds of these ResMed AirSense CPAP machines. I work on the frontline in the hospital, and the wheels are about to come off.
Godspeed!
Can you provide details on how you know the AirSense10 is identical to the AirCurve 10? I’m looking into was of repurposing these devices as well, since they are one of the most common devices around.
So you’re saying the the AirSense10 is in fact a BiPAP machine with firmware that prevents it from being used as such? I’d like to help.
My first focus is creating a filter/UV scrubber to attach to the exhaust manifolds of CPAP masks, to reduce the concern of virus aerosolization when using these machines, but my second would be “unlock” these settings so they can be used as proper emergency ventilators.
James, send me an email to freyrreynir (at) gmail
Forget UV on moving air everyone, it’s like spraying a hosepipe through a candle flame and saying you boiled water. Sure you can eventually boil a small amount of water with a candle flame, but to insta-boil the water needs something on the scale of a rocket engine, so the candle equivalent UV bulbs are not going to do it, you need the rocket engine equivalent UV source to instantly sterilise the air. No, still more power than you’re thinking, you haven’t got the circuit capacity in your house to run it, neither does the average hospital ward.
Your typical UV “candle” can sterilise surfaces with long exposure times though.
An Iron lung has been built in 10 hours with two oil barrels and vacuum cleaner and wooden valves in 1949.
https://books.google.com/books?id=giQDAAAAMBAJ&lpg=PA2&ots=Nw4rQxjsnI&dq=popular%20science%201949%20october%20iron%20lung&pg=PA126#v=onepage&q=popular%20science%201949%20october%20iron%20lung&f=false
What if we combine an RC flight controller(with a custom loop software), an ESC and brushless motor to rotate a drive shaft, an analog PITOT tube to measure positive and negative pressure from the breathing mask( a cheap CPR mask), a 30g continuous servo to shorten or lengthen the arm that pushes the Ambu bag(regulating thus the maximum output air volume), a buzzer to activate when the pitot tube indicates threshold levels, LEDs to indicate functionality of the ESC/ motor minimum rpm pitot tube levels(like a ruptured amb bag) 3d printed or even wood to make the housing to hold the ambu bag and the lever to push it; would all these readily available components make a ventilator that could assure minimum conditions to help Covid19 patients? Any RC Hobbiist has tones of these parts lying around. My 2 cents. VM, M.Sc.Eng
Why can’t we use c-pap machines for the less critical patients that need respiratory help? Leave all of the computerize whiz bang units only when completely necessary and do the simple no frills c-pap that delivers constant help and doesn’t require pressure in and out adjustments.
Just thinking a common sense approach out lot. Sometimes we can’t see the simple solution betcause the problem is so complex.
CPAP masks aren’t designed to filter the exhaled air. That can be solved, yes, but you need to design new masks at least.
What about using speakers as precision pumps? Eg glue a thin film bag on to a speaker and mount the speaker on a board or something to apply pressure to the bag. Put one way valves on the bag and use a smartphone for some kind of PID loop with some other sensors for flow.
I know its a huge oversimplification but I like the idea because the parts are so readily available. No 3d printing, exotic parts, or highly skilled fabrication required to get an extremely high precision pump. The right software could make it familiar and easy to use for doctors and nurses.
I had thought of something similar, think about the monitoring sensors as throttle and brake.
Engineer a sound with the correspodending frequency range and use technics like in a simulator (e.g. engine sounds).
Use the same phone to interpret the sensors in an app and to influence the base frequency or other modulaties.
It would need
a mobilephone,
an amplifier and a speaker which could be connected to
a tube / pipe / pet-bottles,
maybe another membran, depending on the speaker.
and the stuff that is needed in other ideas too, but is not replaced with the above.
the low amplitude of the motion could maybe countered with more surface in the volumetric vessels?
Looks like the Turks already got very serious prototype. https://twitter.com/Selcuk/status/1244661929777532930
I like the idea of adding o2 directly to ones blood. It seems like a good temp fix. I also like the idea of draining the fluid in a patient’s lungs, if that is possible. My main idea is to build an air cleaner / virus zapper to clean the air in hospitals, supermarkets, cars, homes and air from ventilator patients. I’m thinking input air, heat to some temp like 250 deg, add back mosture and recirculate.
I don’t agree about recirculating air that is contaminated. Why take the risk when it could go into an incinerator, separated right at the mask or face apparatus.
“adding o2 directly to ones blood” is almost the concept of ECMO, above.
It’s off topic from a ventilatior, but I bought a bottle of Everclear and Grey Goose Vodka and have been researching inhaling ethyl alcohol via vapor. WOW…do in moderation. I used some to hand sanitize and took a smell to get used to it. It about knocks you over. A few drops in a face mask would go a long way….all in moderation. I can’t imagine a better anti-viral.
I took about a 10 minute “treatment” of the vapor. It gave me a head rush but other than smelling it for a few hours, had no noticeable bad side effects. This morning I am clearer than normal, but it’s way to soon to make any conclusions. Since it is very addicting, I will continue a daily treatment through April …..and stop cold turkey the first of May.
It seems to me that this is a viable treatment that could be very effective in the early stages. A very small amount could be introduced into a ventilator also. A drop on a face mask may be viable for some people.
Feeds salt water into converter to make it into oxygen for professional divers testing it on land even with dirty swamp water after making an ai chip to id it via sniffing it and other harmful things to filter out the bad into a dumping unit in the chemical conversions of water to oxygen sort of like for smokers with throat cancer needing a portable respirator as it cleans it for them.
I think the Mechanical Ventilator Milano (MVM) should be mentioned here as well. I discover the novel ventilator design as I was browsing Adafruit’s Instagram.
Mechanical Ventilator Milano (MVM): A Novel Mechanical Ventilator Designed for Mass Scale Production in Response to the COVID-19 Pandemics
https://arxiv.org/abs/2003.10405
Submitted 23 March 2020
Worth a look before wasting resources, issues with low cost ventilators https://www.youtube.com/watch?v=7vLPefHYWpY&t=325s
Great brainstorming discussions here… I haven’t see a single “A.I.” being mentioned here. I was wondering whether it is possible to implement the A.I. technology into ventilator machine. So the learning machine are able to make adjustment on level of oxygen flow matching the patient’s breathing capacity. Just wondering…
having personally experienced bronchitis and pneumonia multiple times since i was about 1 years old. until about the age of 12. i did not have a ventilator but survived on my own. I soon found that your lungs fill with a mucus liquid that hampers breathing. My solution was to hang over the side of my bed, over a pot of steaming hot water, and actually drain my lungs into the pot. for a few hours every day. ..it required a distraction as it tickles your lungs to be drained. so i read a lot, upside down. After a few weeks it reduced to a cold. and then disappeared. A few things happened over timed , my total lung capacity increased by about 1/3 total volume. i learned how to survive off puffs air using only the tops of my lungs. or special skills. I also never slept flat on my back or both lungs would fill, so one side or the other, In summary i think the focus should be on draining the mucus out with gravity assist, and then consider ventilators . they sure would have helped, One other thing i found, i could avoid catching this cold family virus by avoiding a chill by wearing a under shirt, even if i was sweating and went out side i was fine…..but without it i could guarantee another round of sickness. …..not sure why but worth mentioning. I hope this helps you , i seem to see the elephant in the room…..its drainage……
Larrie Cole
Inventor and eng.
Helmet-based ventilators may be far superior according to studies at University of Chicago Medical Center, see https://www.helmetbasedventilation.com/about. 2016 study concluded: https://www.uchicagomedicine.org/forefront/patient-care-articles/helmet-based-ventilation-is-superior-to-face-mask-for-patients-with-respiratory-distress
All-pneumatic (no electricity) ventilator can be built from kit from off-the-shelf industrial parts, in the process of safety testing now: http://MakerVent.com/gallery