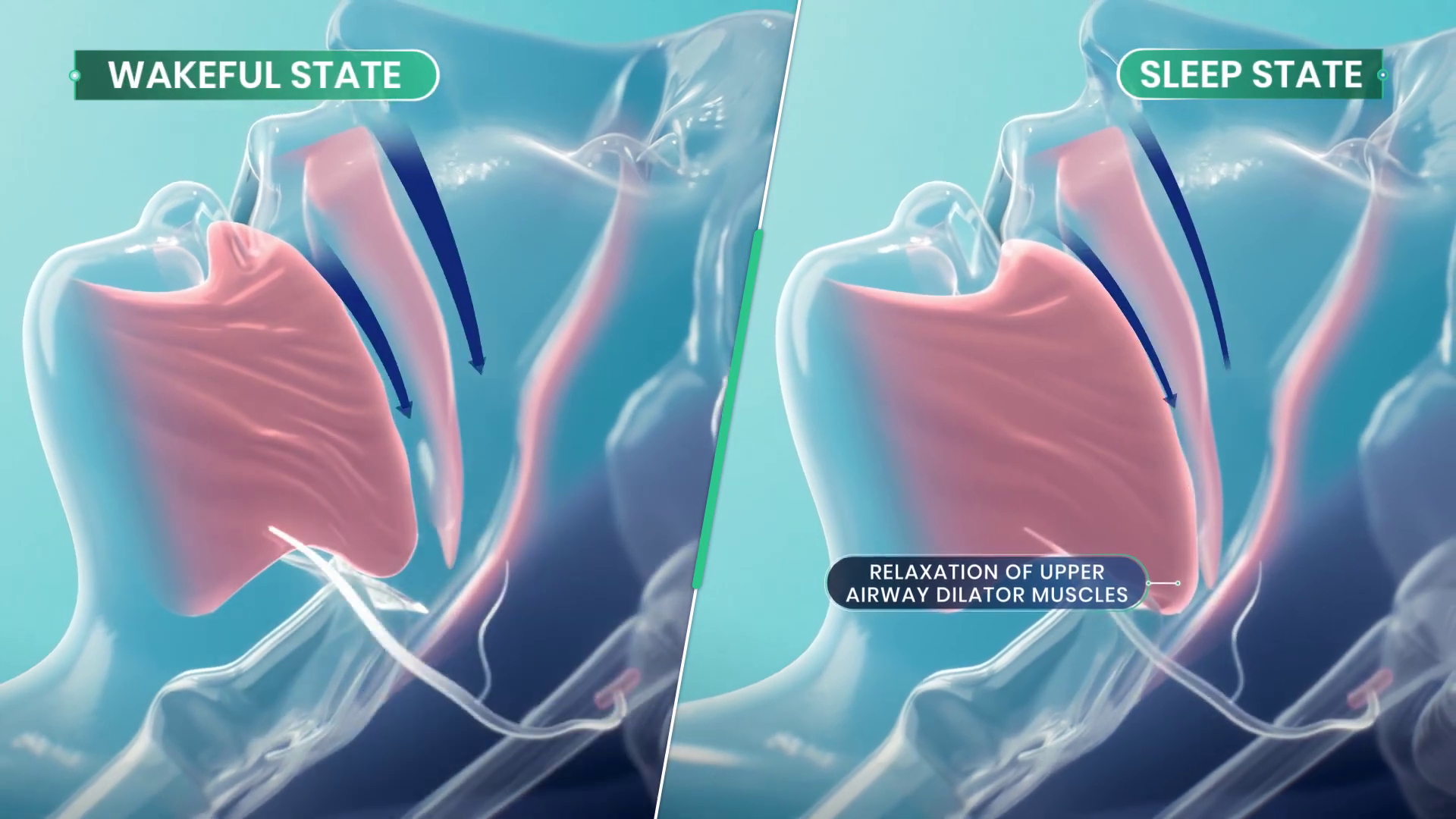
Sleep apnea is a debilitating disease that many sufferers don’t even realize they have. Those afflicted with the condition will regularly stop breathing during sleep as the muscles in their throat relax, sometimes hundreds of times a night. Breathing eventually resumes when the individual’s oxygen supply gets critically low, and the body semi-wakes to restore proper respiration. The disruption to sleep causes serious fatigue and a wide range of other deleterious health effects.
Treatment for sleep apnea has traditionally involved pressurized respiration aids, mechanical devices, or invasive surgeries. However, researchers are now attempting to develop a new drug combination that could solve the problem with pharmaceuticals alone.
Breathe Into Me
There are a variety of conditions that fall under the sleep apnea umbrella, with various causes and a range of imperfect treatments. Perhaps the most visible is obstructive sleep apnea (OSA), in which the muscles in the throat relax during sleep. Under certain conditions, and depending on anatomy, this can lead the airway to become blocked, causing a cessation of breathing that requires the sufferer to wake to a certain degree to restore proper respiration. Since the 1980s, OSA has routinely been treated with the use of Continuous Positive Airway Pressure (CPAP) machines, which supply pressurized air to the face and throat to forcibly keep the airway open. These are effective, except for one major problem—a great deal of patients hate them, and compliance with treatment is remarkably poor. Some studies have shown up to 50% of patients give up on CPAP treatment within a year due to discomfort around sleeping with a pressurized air mask.
Against this backdrop, a simple pill-based treatment for sleep apnea is a remarkably attractive proposition. It would allow the treatment of the condition without the need for expensive, high-maintenance CPAP machines which a huge proportion of patients hate using in the first place. Such a treatment is now close to being a reality, under the name AD109.
The treatment aims to directly target the actual cause of obstructive sleep apnea. OSA is a neuromuscular condition, and one that only occurs during sleep—as those afflicted with the disease don’t suffer random airway blockages while awake. When sleep occurs, neurotransmitter levels like norepinephrine tend to decrease. This can can cause the upper airway muscles to excessively relax in sleep apnea sufferers, to the point that the airway blocks itself shut. AD109 tackles this issue with a combination of drugs—an antimuscarinic called aroxybutynin, and a norepinephrine reuptake inhibitor called atomoxetine. In simple terms, the aroxybutynin blocks so-called muscarinic receptors which decrease muscle tone in the upper airway. Meanwhile, the atomoxetine is believed to simultaneously improve muscle tone in the upper airway by maintaining higher activity in the hyperglossal motor neurons that control muscles in this area.
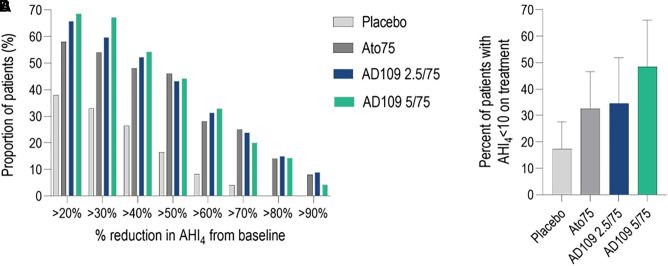
Thus far, clinical testing has been positive, suggesting the synergistic combination of drugs may be able to improve airflow for sleep apnea patients. Phase 1 and Phase 2 clinical trials have been conducted to verify the safety of the treatment, as well as its efficacy at treating the condition. Success in the trials was measured with the Apnea-Hypopnea Index (AHI), which records the number of airway disruptions an individual has per hour. AHI events were reduced by 45% in those taking AD109 when compared to the placebo group in a phase 2 trial featuring 211 participants. It achieved this while proving generally safe in early testing without causing detectable detriments to attention or memory. However, some side effects were noted with the drug—most specifically dry mouth, urinary hesitancy, and a level of insomina. The latter being particularly of note given the drug’s intention to improve sleep.
Testing on AD109 continues, with randomized Phase 3 trials measuring its performance in treating mild, moderate, and severe obstructive sleep apnea. For now, commercialization remains a ways down the road. And yet, for the first time, it appears promising that modern medicine will develop a simple drug-based treatment for a disease that leaves millions fatigued and exhausted every day. If it proves viable, expect it to become a major pharmaceutical success story and the hottest new drug on the market.













As someone with sleep apnea, an AHI of 10 or less is not what I’d call good. The usual goal is 5 or less. That’s an average of 5 apnea events (obstructive apnea or hypopnea) per hour.
At that level, doctors will consider your apnea treated.
At that level, your sleep will still be fragmented and you will still have fatigue and other symptoms.
An AHI of 10 is far outside of what is considered good treatment. The range for mild sleep apnea is 5 to 15, so 10 still counts as having sleep apnea
I can see it used in parallel with APAP treatment to reduce the required pressure. I don’t see it replacing APAP, especially given the side effects.
From what I see on various forums and social media sites, a large part of the reason people quit APAP comes down to a few reasons:
Unrealistic expectations. Folks expect to wake up after using APAP, and feel like they’ve been reborn. Very few actually have that experience. For me, it was a long, slow, almost imperceptible improvement. It was most noticeable in that my consumption of Coca Cola went from 5 liters per day to stay awake and functional down to just drinking it now and then because I like the flavor. That was spread literally over years.
Insufficient support. Finding a well fitting mask is regarded as close to black magic. APAP machines are often delivered with the pressure settings left at the full available range. People need more assistance in properly adjusting the masks – much of the problem with masks isn’t that they don’t fit, it is that people don’t know how to adjust the headgear that holds it on your face. The wide open settings are are starting place, but not an adequate prescription. After a few nights on the wide open settings, you need to read out the full data from the machine and raise the minimum to a level that fixes most of the apneas. You also need to check for therapy emergent central sleep apnea (TECSA.) TECSA causes apneas that cannot be treated with pressure – you actually have to reduce or limit the pressure to keep TECSA from getting out of hand. TECSA does tend to get better with time, requiring periodic changes to the pressure settings to better treat the obstructive apnea as the TECSA goes down. All of that requires assistance from a trained technician or that the user takes charge of the treatment and changes settings as required. The user needs to have that explained and understand that it will all take time.
There are, of course, people with neurological or psychological problems who have difficulty with having something in contact with their faces while trying to sleep. Those folks need more assistance than the average user – and they don’t often get it.
There is more to acceptance, of course, but there’s only so much of it you can squeeze into a comment.
At any rate, I see the pills as helping with PAP treatment rather than replacing it.
As someone who recently learned of their apnea, I can relate. The machines are frustrating and I’m already on my second mask trying to get a right fit. I have what they call “mild” – which is anywhere from 20-30 AHI events an hour for me. I still have insomnia and narcolepsy symptoms. It’s definitely support, but not a silver bullet.
How to measure AHI events? (55 yrs old, some kg more than my ideal, no sleep igiene, snoring, my wife try to keep me alive awakening me when she say “you was not snoring or breathing” 😆). But
The best thing to do is go to a doctor for a sleep study. I was first given a take-home device that I wore for one night for diagnosis, and then did an in-office overnight sleep study (wherein they tested air pressure levels while I slept to find the right settings for me).
Record your Photoplethysmogram for both Red and IR channels. Estimate SpO2 and heart rate. Count HR spikes of ~30BPM with SpO2 dips of >3% or so. Those are arousals from the lack of oxygen. Count how many in an hour. That’s your AHI.
You can purchase SMD dual LEDs (Red+IR) on LCSC, as well as an SMD phototransistor without filter.
Go to the doctor, I’m now using mine since 2021, even my wife’s sleep is better.
Btw, I had a severe (>120 AHI) and for a lot of years this condition not being treated, I was told (by neumonologist and heart specialist doctors that this produces arrhythmia) that this contributes to the heart doing some misfiring (when the brain is without oxygen, it sends an alarm to the heart and the heart change its rhytm to act accordingly), That’s is in not tecnical/medical terms what they told me, how much that is true or not I don’t know. It’s true that there are false expectations, about being like a reborn when you start using some kind of machine, but I could tell, that, using the machine when I was confortable and was tweaking settings, the same machine recorded much much better results. Today I have a monthly average of 0.7 AHI. Let me also suggest low contact/friction masks, I’m in love with one mask brand/model in particular, one brand that I’ll would not buy the machine (there were some issues in some cheap components that weren’t suitable for the task), this brand made also, ICs, Audio Equipment, lightbulbs, etc, its a wide spread and old brand, you will know when you do your research. Also this mask is good if you happend to breathe with your nose, some people need a full face mask, I don’t know how that would work. Reading at the note itself, seems that I was one of the lucky that can use a respirator machine, but let me tell that if you can by other means solve this issue, it would be great, going to camp, to holidays, a weekend with friends and having to go with an extra bag is no fun.
Get a sleep study, really. Wives are primary detection units, and if they say you’re not breathing, you have sleep apnea.
If you must have evidence before you seek medical attention, https://www.amazon.com/Bluetooth-Health-Tracker-Overnight-Saturation/dp/B094JG4JD7
It will show your oxygen starvation at night, and the app does not require a cloud connection to operate.
There is a great Android app called Snore Lab that records the noises you make and listen back. Combine this with a smart watch that records Sp02 levels and you can hone in on when to listen in the recordings.
This is what I had to do to get an NHS GP to take it seriously. They said doing the test was a waste of time, but once I had the evidence they couldn’t deny the test, which after over a year sitting on a waiting list came back as severe!
and do the exercises! Snore free, snore gym, whichever. They have a tremendous effect, except once you stop doing the exercises, it comes back.
Problem is doctors can’t prescribe exercises and people don’t want to do them.
With that massive amount of sugar or just drinking so much fluids, wasn’t that actually contributing to the problem?
When I’m drinking a lot of soda, I get bloated and my throat gets stuffy.
Also, there’s something about sugar in candies and sugary sodas that makes my throat close up slightly. Makes my voice “difficult” for a lack of a better word. Maybe it’s the osmotic pressure or the acidity, or something that irritates the tissues. I can imagine constantly consuming cola would have an effect.
Oddly enough, now that I am not drinking that amount of liquids a day, I have more trouble with water retention. My feet and legs swell these days. They did not do that back when I was drinking 5 liters of coke.
It turns out that drinking more water actually reduces edema.
In getting my apnea under control, I’ve found that I have to keep the swelling from edema down. Right now, that involves taking a diuretic, wearing compression stockings, and drinking more water during the day. I’m also working on reducing salt.
Could it be that it flushes out excess salt? Too much salt intake results in the body trying to compensate by holding on to liquids.
Yep. You have to drink enough to dilute the salt so it can be washed out. That has the side effect of washing out other minerals and stuff that you need.
I’m working on reducing salt and taking tablets to replace the potassium that gets washed out with the salt.
Between the diuretic and drinking more water, my potassium levels were so low that the doctor in the hospital couldn’t use a general anasthetic for the operation when I broke my leg in November. They had to use local anasthetic and some kind of neuroblocker for the pain and something to make me sleep. They held off on the operation for a day or so while giving me potassium through an IV to build it up to a safe level.
I’m of the opinion that the potassium deficit was the cause of the broken leg – I had been having trouble holding and carrying things and had been somewhat wobbly in the knees all day before tangling with the small trailer that ended up breaking my leg – which happened when I slipped while pushing the trailer a few feet into position to unload it. The low potassium levels would explain the weakness and the wobblies.
It all ties together in a big mess.
After 3 months of trying, I put the machine back in the box and send it back. It just wasn’t worth it. I can’t deal with it. I can only sleep in the recovery position and the facemask just hurts. Besides that, the forced air is incredibly annoying, the machine noise (was the most quiet model of 2023) is annoying, it makes my adrenaline go through the roof. Trying to sleep in a fight or flight mode that keeps going, doesn’t work. Tried it for 2 hours a night and it made me so tired, I had problems staying awake at work. Made me cranky, made me fall sleep at bad times during the day. It was a disaster.
My “solution” is to put my right hand under my ear so my head falls forward on my pillow. I use a stiff pillow. My head tilts slightly down and I can sleep perfectly fine like that. If I move during the night, I wake up and move. I sometimes switch to my right side and it’s something I know I actually do and I put my other hand there.
Saving you all from yourselves – Sleep Bastion anti-snore silicon nasal vents. They looks like little silicon golf ball baskets that you shove up your nose and it keeps your nose from closing at the pharynx by opening the muscle higher up at the back of the septum. come sin a 12 pack for $15 and you can use them for months before they wear (yes wash them you goblin).
Seems dubious, why would forced opening near the entry of the airway eliminate the rest of the airway closing due to relaxed musculature?
Should be combined with sleeping pill and ear plugs so no external perturbances will awake you.
Sleeping pills is to be taken very sporadically.
It’s not a good long term solution at all.
Sewing a tennis ball on the back of your sleeping shirt on the other hand prevent you from sleeping on the back, and can help a lot.
I was sure insomnia would be a side effect, just from reading the method of action.
Well I think insomnia and sleep apnea rarely occur together.
You would be surprised.
Some people are so exhausted from fighting the tiredness all day that they have trouble falling asleep.
Some have to use so much caffeine to stay awake that it prevents them from falling asleep.
Some people get depression from the tiredness, and that causes insomnia – worsening the tiredness in a vicious cycle.
I got sleep apnea. I’m so tired in the morning. Extremely tired. If I have a meeting before lunch I have trouble staying awake. Sort of awake in the afternoon. In the evening I’m ready to take on the world. When I need to go to bed I’m awake like i just finished a supertanker full of redbull.
Try snore gym app and Snore Free. Works for me unless I stop. Try it for at least two weeks. My dentist actually recommended it.
Aren’t the majority of sleep apnea patients overweight? It seems like weight loss would be a much better strategy than something which has a high potential to interfere with the quality of sleep.
I’m not overweight and have been using cpap for over a decade tyvm you insensitive clod
‘majority’ isn’t the same as ‘everyone’ and I fail to see how pointing out a potential treatment for the majority of sufferers, especially one that comes with so many other benefits is ‘insensitive’.
Perhaps not obvious to those not lurking in the wrong places many years ago, but I strongly suspect that was meant in jest. You can google the phrase for a little background :)
I am 5 feet 10 inches tall (180cm.) I had apnea back in the days when I weighed 130 pounds (60 kg.)
Overweight is one cause of apnea, but not the only cause.
Some of us were simply born with narrow airways.
Certainly and, for those with atypical presentations, I understand the need for other treatments.
According to some random web results, less than half are overweight. And AFAIK weight loss does not always fix sleep apnea even if weight gain had originally triggered it.
I’d suggest looking at the articles, the summaries can confuse it. While the majority of overweight and obese individuals don’t have OSA, the majority of people with it are and weight loss has a high success rate.
not only, person with Pierre Robin syndrome are also impacted by apnea. though not sure if this drug could help, as it is more genetic/physiologic.
Depending on whose studies you look at, five years after starting a weight loss program, 85-95% of people have regained all they’ve lost. Numbers are much better for surgical weight loss: there only 40% of people have regained the weight they lost, but people who qualify for weight loss surgery are uniformly obese and post-surgery less than 5% of them are no longer obese, they’ve just managed to maintain the weight they lost post-surgery.
So any plan that starts with “well just do this thing that has less than a 10% chance of working” is probably not going to have good results.
My genetics predispose me to being quite skinny, but my sustained and vigorous attempts to get from 8% subcutaneous fat down to 4%, over a period of 20 years of bike racing, were met with my body doing all sorts of interesting things none of which yielded a sustained sub-5% body fat percentage.
Agreed, weight loss is hard those statistics paint an unfairly grim picture because they lump dietary fads in with sensible strategies like caloric monitoring.
Nope. I am not overweight. I also don’t eat lactose, gluten or caffeine. Weight has nothing to do with it. Read the article – it’s neuromuscular.
Apart from the other excellent replies, this question was answered in the article pretty clearly i thought. The reason they are looking for a drug as an alternative to CPAP is that some patients do not comply with CPAP. Guess what, they don’t comply with weight loss either. An effective cure relies on meeting people where they’re at, that’s why magic pill solutions are so well-loved.
Even for those who are overweight, sustained weight loss is not something that we (medical science) know how to do reliably. So it is a strategy of limited usefulness. What good does it do to say to do something we don’t know how to do in practice?
(Increased activity and healthy diet have many benefits and are worth pursuing as general mission, but they are unlikely to yield prompt, lasting relief from acute sleep apnea issues.)
In some cases, addressing the apnea may help enable greater activity to address muscle tone or weight issues. (It may be tempting to blame apnea on weight, but the relation may be more complex, or may be coincidence.)
There is some evidence that singing can help reduce obstructive sleep apnea some.
CPAP machines are ridiculously overpriced $2,200-$3,000 because of the huge markup and partial insurance coverage. Sleep clinics are really all about selling a CPAP machine for profit and rewards, they push for it.
I’ve done a few sleep studies with crapola Resmed monitors.
First one, tubing was already damaged, kinked so that pressure sensor (by armpit?) read nothing.
Second one, batteries went dead after about an hour.
Third one, when picking it up, I noticed tubing was already damaged, hose kinked so I complained and they fixed that on the spot. But the tubing fell off me (not enough tape) and it did not apparently test for the 4 hrs required. They are a bulky, stupid design.
I tried a Resmed 10 and found you could not set the peak-peak pressure, it was always too close. Gave up and now the loss of brain cells is slowly putting me on par with the apes.
I lucked out I guess. Starting a CPAP had a dramatic effect on my sleep (and wakefulness) in a couple of days. I tolerate the mask well and I’ve used it every day for the last 15 years. I don’t think it affected my weight.
My original F&P gave out after 12(!) years and I got a new APAP. I ended up fighting it during the night so I turned off all the fancy features and run it as a basic CPAP. It took a while for the insurance to come through for the new machine so in the meantime I built my own out of a PWM module and a 12v fan in a cardboard box, and used the hoses I already had. It was noisy but “white” noisy so I didn’t mind it.
Please write it up, I might be interested in building one myself as a stopgap before the healthcare system delivers.
Or at least tell us what kind of fan.
It was beyond basic and all from Amazon. It was a 12v impeller/blower fan with a round output vent, and a motor speed controller. I 3D printed an adapter for the fan output to the hose size but you could duct tape it up just as well. I put it in a cardboard box lined with dishtowels to damp the noise a bit. I spent a few nights adjusting the speed to the minimum required to do the job. It was that simple and surprisingly effective.
The very first PAP machine was made out of a vacuum cleaner. It was used to help a dog with respiratory problems breathe.
The first one used on a human was made from a compressor.
Both were crude, both were useful.
https://www.apneamed.org/blogs/info/the-history-of-the-cpap-machine-technology-today
Ah, a “new drug”…..fine print:
May cause osteoporosis, blindness, cardiac arrest, leprosy, hair to fall out, hearing loss, impotence, memory loss, swelling of lymph nodes, hallucinations, suicidal thoughts, and in rare cases death. Use only as prescribed.
Left out, diarrhea and constipation. American spelling. Both at the same time?
You left out “Don’t take this drug if you are allergic to it.” 😁
It’s not even a new drug, just a novel combination. Side effects are likely to be the limiting factor with this combo…
Forgot oily discharge
I have a suspicion that the proliferation of wisdom teeth surgery and tooth extractions are causing bone loss in those mandible and sinus areas, leading to the collapse of those soft tissues in that area and the rate of sleep apnea patients we are seeing nowadays. I’m willing to guess sleep apnea wasn’t as common back in 1850 when we (US mostly) had better diets and didn’t perform unnecessary, dangerous and unfounded cash grab surgeries eg. wisdom tooth extractions, tonsil removals, and circumcision.
On the other hand, diseases of nutritional deficiency were more common then. Tooth loss, due to inferior oral hygiene, and less use of flouride were much more common. Most people were more immediately exposed to smoke and combustion products (from lighting, heat), which tend to irritate airways.
People with obstructive sleep apnea are more likely to get respiratory diseases, like pneumonia, influenza. They also are affected more severely. Before antibiotics and vaccines, communicable disease killed a much larger percent of the population at a much younger age than they do now. It would not be surprising if a smaller portion of the population had sleep apnea, because those with it died sooner.
If this causes sleep apnoea you REALLY should talk to a professional ASAP.
On one side: I had relatively little trouble adapting to a CPAP nasal mask. Yes, it was a nuisance for a while, and I may be better about compliance than many, but I suspect many actually give up on it before giving themselves a chance to adapt to it.
On the other side: I was on an SNRI when diagnosed with sleep apnea. Admittedly, the S stands for selective, and a different drug might indeed have different effect. But it does make me a trifle skeptical about this new treatment.
SNRIs are pretty much designed only to alter norepinephrine levels in the brain. That’s not what “selective” means in the name, but: “in the rest of the body, norepinephrine increases heart rate and blood pressure, triggers the release of glucose from energy stores, increases blood flow to skeletal muscle, reduces blood flow to the gastrointestinal system, and inhibits voiding of the bladder”-W. People are sadly misinformed about how such hormones/neurotransmitters play a variety of roles. For example there are 14 different serotonin receptors in the body and five different dopamine receptors, but still bro-science will insist on practices and substances raising or lowering “dopamine levels”. Ask a Parkinson’s patient about the effects of low dopamine levels. It’s much, much more complex than what self-help gurus suggest.
Anecdotally i can confirm that atomoxetine alone does treat sleep apnea. The side effects aren’t worth it for me though.
One notable line from the paper is the following: “Atomoxetine taken alone decreased total sleep time (P < 0.05 vs. AD109 and placebo).” Based on that, the data in the paper, and my own experiences, I think the aroxybutynin might not play any therapeutic role. Instead it serves two other purposes: it alleviates some of the insomnia caused by the atomoxetibe by making people feel drowsy, and it allows the manufacturer to patent a new drug combination that they can then claim provides clinical benefits that are not available by taking atomoxetine alone. See Auvelity for another example of this: it’s identical to taking bupropion and dextromethorphan together, but by putting both in the same pill they can patent it as a new drug.
Probably you’d get the same results by just taking atomoxetine and any other anticholinergic; there doesn’t seem to be anything special about aroxybutynin except for the fact that it’s a novel drug. My understanding is that it’s not good to take anticholinergics chronically though, so I’m not sure how much sense it makes to treat sleep apnea with this drug combo when one of its constituents might cause the same problems as sleep apnea itself.
Today I learned that apnoea / apnea is yet another word where Americans have dropped a letter.
American and British spellings for medical terms began diverging noticeably in the early 19th century, driven by American spelling reforms.
Origins of Divergence
Early 18th-century English spelling was inconsistent across both regions, but Samuel Johnson’s 1755 dictionary standardized British forms with diphthongs like “oe” and “ae” (e.g., “foetus”, “haemoglobin”) to reflect classical Greek and Latin etymologies. An 1814 American medical text still used British spellings such as “tumours” and “centres,” indicating overlap persisted initially.
Key American Reforms
Noah Webster’s dictionaries (1806, 1828) simplified spellings by dropping “oe/ae” to “e” (e.g., “fetus”, “anemia”), favoring phonetics over etymology, a trend accelerating in the 1820s-1920s. Medical adoption followed, with U.S. texts shifting to “hematuria” by the 1920s while Britain retained “haematuria”.
Modern Persistence
British medical English clings to traditional forms in journals like BMJ, but global standardization often favors American simplicity; both coexist without strict rules.
Surprised no one has mentioned Didgeridoo playing, training and practice, there’s been published medical research papers which found it functions like a therapeutic workout for the muscles and results in measurable improvements for people with snoring and sleep apnea problems.
I was diagnosed with 25 AHI in 2016. After my first night with a CPAP, it felt like being newborn again. Then came a long struggle with masks. I ditched all face masks and started using one that goes under the nose (nasal pillow mask). The only problem, I opened my mouth during sleep. I began taping my mouth with medical tape (one or two strips across). I did this for six months and after this I’d learnt to sleep with my mouth shut. Nowadays it happens rarely that I’ve opened my mouth during sleep, so it’s not an issue. I’ve used the CPAP now for 10 years, every night except one. Fortunately, I’m in Europe, so the CPAP and masks are “free” (paid for by my tax!).