The news these days is dominated by the one big story: the COVID-19 pandemic. Since the first reports of infection surfaced in China sometime in late 2019, the novel coronavirus that causes the disease, bloodlessly dubbed SARS-CoV-19, has swept around the globe destroying lives, livelihoods, and economies. Getting a handle on the disease has required drastic actions by governments and sacrifices by citizens as we try to slow the rate of infection
As with all infectious diseases, getting ahead of COVID-19 is a numbers game. To fight the spread of the virus, we need to know who has it, where they are, where they’ve been, and whom they’ve had contact with. If we are unable to gather the information needed to isolate potential carriers, all that we can do is impose mass quarantines and hope for the best. Hence the need for mass COVID-19 testing, and the understandable hue and cry about its slow pace and the limited availability of test kits.
But what exactly do these test kits contain? What makes mass testing so difficult to implement? As we shall see, COVID-19 testing is anything but simple, even if the underlying technology, PCR, is well-understood and readily available. A lot of the bottlenecks are, as usual, bureaucratic, but there are technical limits too. Luckily, there are clever ways around those restrictions, but understanding the basics of COVID-19 testing is the best place to start.
Going Hyperbolic
Currently, the only way to detect an active SARS-CoV-2 infection is by the use of polymerase chain reaction, or PCR. We’ve covered PCR in some detail before, but briefly, PCR is a laboratory method that relies on the cellular machinery that allows DNA to replicate itself. PCR is a three-step process:
- Denaturation, which uses high temperatures to break the hydrogen bonds between base pairs in the DNA double helix, creating complementary single strands of DNA;
- Annealing, which occurs as the temperature of the reaction is lowered and short oligonucleotide primers, specific for a section on the target DNA, bind to the single strands;
- Extension, where the DNA between the primers is filled in by an enzymatic reaction. The result is a double-stranded DNA segment, which then goes through subsequent rounds of denaturation, annealing, and extension, resulting in exponential amplification of the specific target DNA.
If the DNA you’re looking for is present, the PCR process will amplify it to a large enough amount that it becomes easy to detect. If what you’re looking for is absent, it will not be amplified and it becomes equally easy to note its absence.
Molecular biology techniques in general, and PCR specifically, are incredibly powerful and flexible technologies. In the case of viruses like coronaviruses, that flexibility is advantageous because the viral genome is contained in a single-stranded molecule of RNA rather than DNA. Detecting the presence of the viral RNA in a patient sample, which is generally a throat swab containing viral particles expelled from the lungs and pharynx, requires first isolating the RNA, then turning it into DNA with the enzyme reverse transcriptase. That DNA is then amplified using PCR.
In either PCR or RT-PCR, detection of the amplified DNA region is accomplished by tagging the reaction with fluorescent probes. The probes bind nonspecifically to DNA, and when produced in abundance by PCR generate an easily detected signal. In actual practice, the kinetics of the PCR reaction are monitored by measuring the fluorescence after each cycle of PCR. This is known as quantitative PCR, or qPCR; when couple with reverse transcriptase, the process is called RT-qPCR.
PCR’s ability to detect the specific genetic signature of SARS-CoV-2 relies on the use of carefully selected primer oligonucleotides. Using the viral genome data published by the Chinese in January, the main primers were designed to amplify the genes coding for two viral encapsulation proteins. Along with those are primers for all SARS-like coronaviruses, as well as a primer for a human gene that should always be present, which acts as a positive control to make sure the reaction worked.
It’s In The Environment
Like any diagnostic or therapeutic technology, testing for COVID-19 is tightly controlled by regulatory agencies around the world. As frustrating as the delays caused by the necessary certifications may be, they’re understandable given that human lives are at stake. An emergency situation such as the current pandemic no doubt will relax some of those bureaucratic necessities, but they’re not likely to be eliminated entirely. Still, the simplicity of PCR and the availability of the reagents and instruments needed to perform the test are tempting targets for biohackers who are eager to do their part.
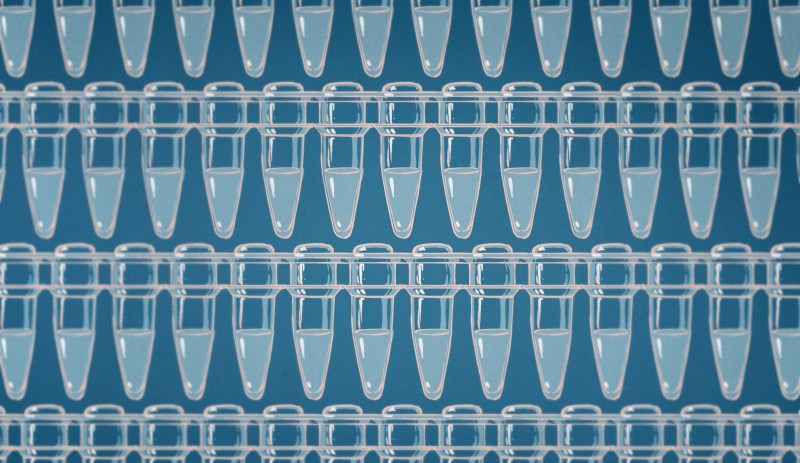
Fortunately, there’s a large unmet need for environmental testing that biohackers can pursue. Chai, a biotech company in Santa Clara, offers a low-cost, open qPCR instrument that’s capable of the exact kinds of protocols being used for human coronavirus testing. The instrument uses a Beagle Bone Black and while it is not cheap at $5,000 or so, it’s an order of magnitude less expensive than commercial, certified qPCR machines. Chai is currently marketing “environmental test kits” that can be used to swab doorknobs, desks, or other hard surfaces that might harbor droplets from an infected patient’s cough or touch. Thanks to PCR’s signal amplification ability, the samples can contain as little a single copy of the viral genome and still be detected.
Chai is clearly not playing games here and specifically caution against use with human samples. They are strictly in the environmental testing market, but that’s a good thing. Coronavirus can only get into the environment once it escapes from a host, and the virions can only survive for a limited amount of time away from a host cell. That makes environmental testing an excellent proxy for the viral load of the humans in that environment, and can be used to get an idea of the dynamics of that load over time. By making relatively cheap qPCR tests possible, Chai is offering a backdoor solution to the problem of limited human testing.
It’s unlikely that human COVID-19 testing via RT-qPCR can be made to go much faster than it already is. Even when the logistics problems regarding the manufacture and distribution of test kits are solved, there are only so many certified qPCR machines to go around, and only so many technicians to run them. Add to that the likelihood that the techs themselves will get sick, and human testing can only proceed so fast. Innovations like drive-through testing are only intended to protect health care workers and the testing environment (since the throat swab often causes patients to cough, drive-through testing where the patient only cracks the car window means a cough doesn’t contaminate an exam room). And such testing will only increase the number of samples that need to be processed.
Despite these challenges, the availability of PCR as a diagnostic method has been a boon to epidemiology in general and the fight against COVID-19 specifically. And if others follow Chai’s lead in environmental testing, with any luck we may soon see a flood of new data that will reveal the true scope of this pandemic and finally let us start making some headway against it.












This article actually leaves out a huge part of the testing problem: these are only testing for the presence of the virus. They’re not serological tests: that is, they don’t test for *antibodies* against the virus, which indicate that someone was infected, and has some level of immunity to the virus.
Testing for the presence of the virus at this point isn’t terribly useful in the hardest hit communities. The problem is that the serological test doesn’t exist.
To clarify I should say that the serological test doesn’t *widely* exist: there are a few tests out there in labs and in the experimental phase, but it’s certainly not mass production scale like the presence test is.
I didn’t cover it because as far as I could tell, it doesn’t exist yet. I’m doing a follow-up article on antibody agglutination testing and will include anything COVID-19 related.
Is this the sort of test you are thinking of?
New blood tests for antibodies could show true scale of coronavirus pandemic
https://www.sciencemag.org/news/2020/03/new-blood-tests-antibodies-could-show-true-scale-coronavirus-pandemic
Nuclear Scientists Developing Faster, Cheaper Covid-19 Test
https://www.bloomberg.com/news/articles/2020-03-25/virus-test-in-hours-for-under-11-eyed-by-atomic-scientists
Serological testing is need to get more reliable statistics / morbidity and mortality data. It will also play a role in measuring vaccine response and the manufacturing of therapeutic antibody preparations from convalescent plasma. However, testing for the presence of the virus is the most useful in regards to isolation measures and halting the spread. For example – healthcare professionals that had contact with SARS-CoV-2 (PCR) positive individuals typically typically have to keep working- so in many clinics these individuals are then tested on a daily basis and only go into self quarantine if they have a positive PCR result. While not ideal, this is the only way to keep most hospitals running. The same applies to individuals with mild symptoms tested at fever clinics / covid test centers. Positive PCR results = possibilty of viral spread = need for quarantine. The same can’t be said for antibody testing.
One of the reasons this virus is such a bother is because it’s apparently spreading very efficiently, and it can do so only by not causing very serious symptoms – so the visible cases are a tip of an iceberg. The uncertainty about the actual spread is so large that according to a UK study, up to 68% of the population -might- already be infected and just not showing any symptoms.
So it might be that the virus is actually no more deadly than seasonal flu, but because it’s spread so wide in such a short period of time, it’s causing a ton of serious cases all at once, overwhelming the hospital systems and intensive care units. This then shows up as a small number of identified cases, high hospitalization rate, and high mortality because these people can’t be cared for.
It’s an interesting case, because countries like Sweden have decided not to do any special quarantine measures, while most other countries are locking up. If the virus is already spread wide, it wouldn’t matter anyhow because by now most people would have suffered the mild/no-symptoms version and developed immunity.
“However, testing for the presence of the virus is the most useful in regards to isolation measures and halting the spread. ”
We’re *way* past that for the majority of the populated places in the world. For health care workers, sure, but in most other cases everyone should be isolated, period. The serological tests give you people/workers who *don’t* need to be isolated.
“Positive PCR results = possibilty of viral spread = need for quarantine. The same can’t be said for antibody testing.”
At this point “need for quarantine” is less interesting than “no need for quarantine,” which is what the serological test tells you.
This is an interesting and pertinant point!
Unfortunately, the sensitivity and specificity of serological tests typically leave a lot to be desired – often impeding their use. Generally the real performance characteristics of the certified assays are not even known when they enter the market (the characteristics in the “instructions for use” of certified assays are often overly optimistic as they are established using data from a select handful of patients summarized by marketing departments of in vitro diagnostic companies pushing for fast certification). These performance characteristics really need to be treated with skepticism and verified first. Larger studies are time consuming and non trivial – These would require sera from the infected patients (as proven by the “gold standard” pcr data) at different timepoints, and ideally suitably matched negative controls – perhaps using biobanked sera from before the outbreak.
I believe it will be some time before serological tests can adequately guide individual decisions on the return to normal life and work.
best regards,
M. Wakileh
I was wondering what ELISA test(s) were on the market and found this document that covers the different serological tests decent and relating to COVID-19. http://www.centerforhealthsecurity.org/resources/COVID-19/200228-Serology-testing-COVID.pdf
Seems some microbiology labs can offer up their equipment for short term testing if required to streamline the workflow if behind and the validated test method is available. Man…, I won’t go into the self regulated professional industry requirements… amazing to me.
Yay PCR! I happen to work at one of the companies that recently had our COVID-19 45min test approved and it might surprise people but we do a huge amount of testing on our manufacturing environment to ensure that we are clean. You could imagine the importance of shipping product out that is free of all tested DNA. To that effect the amount of biohazard suits used in production to keep peoples skin to themselves makes it look like something out of a scifi movie.
FYI we share our general trending we collect from instrument runs: https://syndromictrends.com/ it’s fun to look at if you are curious what is going around.
Other general words of wisdom as i get to see the gross world we live in on a daily basis. Wash your hands and phones! seriously you a bring a portable toilet with you in your pocket!
Stay clean!
Charles, could you please help us interpret that graph?
The graph is a collection of the rate of what comes up positive on our test from each run test. So in 50% of cases when a test is run in a hospital nothing comes up. this could mean the person has a common cold, allergies or something worse like covid-19. The graph is a depiction of those tests that do come up positive for one or more of the targets tracked. Each test tests for all of those items simultaneously off the one sample collected. So looking at today’s rates if you were symptomatic enough to go to a hospital and be tested there would be a 15% chance of rhinovirus(common cold). This doesn’t mean you don’t also have something else at the same time. In kids for example you may see 2 or more co-infections which is why it is very hard to diagnose properly if a child needs antibiotics or not based on symptoms alone.
Also note the Coronavirus currently listed there is not COVID-19 it is the common cold versions.
You mean SARS-Cov-2?
Yes, Sars-Cov-2 is coronavirus disease 2019 or COVID-19. not to be confused with Sars-COV which is from 2003
Seems like they hire the same guys that give names to USB3.1 Gen2x2. :P
Frankenvirus III: The Plaguening … might have got higher first weekend numbers.
What happened to the Chinese Zodiac or other cult naming conventions? Too obvious source issues?
Hmm, time to break out that junk bin (but still properly enclosed) UV-C germicidal phone bin.
From their web site, Chai claims 1 hour results.
FYI: https://www.scmp.com/week-asia/health-environment/article/3049406/coronavirus-game-changers-hong-kong-macau-universities
>A research team from the Hong Kong University of Science and Technology said on Thursday it had invented a portable detection device that can give a diagnosis in coronavirus cases in 40 minutes, while the University of Macau is working on a kit that may be able to detect the virus in less than 30 minutes, even at early stages of infection.
Hong Kong University of Science and Technology is using PCR.
>The University of Macau is working on a similar test kit.
>“We have been verifying the accuracy of the product with 2019-nCoV samples [the formal name of the new coronavirus] since this week. It is still too early to define the final accuracy, but the initial results are already encouraging,” said Rui Martins, director of the University of Macau’s State Key Laboratory of Analog and Mixed-Signal VLSI.
>The new system, which has been named ‘Virus Hunter’, was developed to detect all types of viruses, including HIV and Hepatitis B, but is being fine-tuned to detect the coronavirus.
>According to Martins, the test kit – expected to be available in one or two months – works by collecting samples of a person’s nasal mucous, which is then placed in a detection chip. The chip is then read by a machine that delivers the final result.
Mologic as well.
https://www.bloomberg.com/news/articles/2020-03-16/ten-minute-coronavirus-test-could-be-game-changer-for-africa
I like the article, but it might be helpful to include the missing first step: reverse transcription, at least as a footnote. It seems to me that a reader who is seriously trying to understand the biology would likely be at a loss as to how the single stranded RNA of the virus becomes DNA in the assay.
You’re probably right. Coming from a biology background, I might have assumed too much. So briefly, the normal flow of information in cells is DNA -> mRNA (messenger RNA) -> ribosomes, which are the organelles that match peptides with the code to create proteins. The process of copying DNA to RNA is called transcription, while reading the code from the RNA and producing proteins is called translation. Coronaviruses and other RNA viruses take over the cell by sending their viral RNA directly to the ribosomes, which short-circuits the other normal cellular translation process in favor of viral translation.
Reverse transcription is the process that some other viruses, called retroviruses, use to make a DNA copy of their RNA genome. HIV is an example of a retrovirus. It happens through an enzyme called reverse transcriptase, which in the case of HIV is stored inside the viral capsid along with a few other proteins and the viral RNA. Once the contents of the virus have invaded the cell, the viral RNA is copied to DNA, the DNA is integrated into the host cell’s genome, and viral replication begins as the cell begins its normal replication process.
Commercial preps of reverse transcriptase are usually modified versions of RT from a leukemia virus called MMLV. Once the reverse transcription is finished, the RT’s job is done. The DNA polymerase used in PCR is generally sourced from extremophile bacteria like Thermus aquaticus, a bacterium from deep-sea thermal vents that can survive boiling temperatures without denaturing.
What is important to understand that the PCR method is the only way currently to reliably test for the presence early in the infection, it is also flexible in terms of mutations. Tests based on antibodies only work reliably after the virus has been around for 9 days or so. For control purposes this is important, as you need to be able to find and control also the asymptomatic patients.
I am building Coronavirus Scanner, which should work real-time to detect coronaviruses on the skin, surfaces.
Just simply spray PCR enzymes over the surface, skin and get the single copy of the coronavirus detected
by electroluminescence effect.
Let me know your opinion and how to contact Chai
You are free to email me one day to join my r&d team
hfexchange at gmail
Hello DJ,
That method may not work. To my knowledge, you would need to use some sort of LAMP assay, these can be quite finicky to get to work since they rely on a stable isothermal temperature to function. Even if it did work, you would be amplifying HUGE amounts of nCoV RNA on the surface of an object upping the likelyhood of detecting false positives.
To my knowledge, you are talking about some sort of LAMP assay. These allow for the amplification of DNA/RNA targets without the need of thermocycling. However, creating HUGE amounts of nCoV RNA on a surface if you detect a positive will increase the likely hood of false positives in the future. I’m not convinced of the utility of this. Not to mention the technical issues of designing an isothermal LAMP assay in the first place.
yeah you would have to heat skin to 94C . I am not volunteering for that.
https://hackaday.io/project/1864-5-dna-replicator
https://hackaday.io/project/6180-dna-lamp-diagnostic-device
Some one should certainly make an easy to manufacture isothermal LAMP device! it is technically simple. A large aluminum block that can maintain a constant temperature +/- 0.5C, and a simple excitation and detection system is all that is needed. Periodic sampling of the reaction will show an increase in fluorescence if real-time detection is required, if not you can run a gel, or do endpoint fluorescence detection to quantify a change in fluorescence indicating that the assay target sequence amplified. real-time quantitative PCR devices are more technically complex. The main trade off is that isothermal devices offload the complexity from the device to the assay, whereas RT-PCR, qPCR, and real-time PCR assays are simpler to develop since it is not necessarily based on tightly controlled/competing reactions. If someone were to make a device that can function with an off the shelf assay Im sure it can do a lot of good right now. My original point was that using Taq polymerase on a surface alone will not yield a functional or useful detection system. It is a good thought however and more people need to be thinking about this!
Theater gel filters can be used as optical band-pass filters that can ensure proper excitation and emission wavelengths from an led source. An LED may be used as the detector as well given a good TIA or a 34S type photodiode. If it wasn’t a conflict of interests for myself I would be pouring designs for these on to the internet right now.
So self enrichment is more important to you than saving lives? I apologize if not, but that’s certainly how your last comment read.
John, I believe that what I and the other engineers/scientists I work with are doing everything we can, as quickly as we can to help a large number of people. We are working 7 days a week and some of us are traveling hours to make it happen. A lot of work and testing goes in to making these devices if they are to be precise. I recognize that in some areas of the world right now, people need detection systems that may not need the ability to finely quantify the samples. There are plenty of open source designs that can fit this niche, the only component of many of these designs that is going to be difficult to find (other than the assay and the sample preparation kits) is the optical filters. That was the main intent behind my last comment.
Here is an example of what to me looks like a good, and relatively simple design that can do some testing fast.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0179133
https://www.flinnsci.com/api/library/Download/3edab69ae1c64e5dbc41d60c2b9a2a7b
Picture an office building. People enter it, get tested: Doorway A, negative results, you leave. Doorway B: you’re infected and automatically jailed (i mean “quarantined”). Point being – wtf good is a “test” for ? the only possible reason is to alert that someone might be a carrier. Aside from that, any positive result is “after-the-fact”.. you’re already infected (if you didn’t already know it from the usual flu symptoms).
Here are some interesting facts from a non-partisan body – puts things in perspective
https://www.cdc.gov/flu/about/burden/index.html
quantitative PCR can be used to track the progress of a given infection, allow a physician to know when someone is recovering or getting worse. It can also allow for discrimination of the virus species and genus, allowing for proper treatment. If the test can be conducted fast enough, you can have extremely precise information for each potential patient allowing the hospitals to stack their resources in the most efficient manner. I agree, you can discriminate purely on manifested symptoms alone, but a lot of actionable information is lost in the ambiguity.
On the high-volume COVID-19 testing front, also check out the work by the University of Washington’s Virology/Medicine Department. They publish their daily and cumulative test results online and have run nearly 27,000 tests of the morning of 25-MAR-2020.
http://depts.washington.edu/labmed/covid19/
The results don’t indicate the source of the samples but I’m assuming these are NOT the general public but instead patients who are either currently infected, those who are likely infected (foreign travel to known hot spots, close contact with known cases), or health workers and first responders.
Per their Twitter feed (@UWVirology), they have capacity for 3,500 tests/day and will be adding more capacity.
It’s SARS-CoV-2, NOT SARS-CoV-19.
The outbreak is called. COVID-19. The virus is SARS-CoV-2.
Hey,
As there is a shortage of PCR equipment and tests all over the world right now I was thinking if a statistical approach to mass testing could be used. My question is: could samples from multiple people be mixed into one and tested. If the test if positive one of them is infected but you don’t know which one. If the test is negative none of them are infected.
This way you could quarantine more people than infected (not together) but could clear more uninfected people. This is also backed by the fact that a small number of tested people are actually infected.
Could this work?
Such an approach could work, but organising would be hard. Yes, mixing samples would work, though the false negative rate would increase also.
They are starting to do this in a county in Romania.
The idea is from Israel where they test 32 or 64 samples at once. If the test is positive they further divide the pool in 2 and test. Seeing that almost 90% of tests are negative this saves a lot of time in testing.
https://www.israel21c.org/israelis-introduce-method-for-accelerated-covid-19-testing/
Found this article looking for the user manual on the Chai kit that finally arrived today. I’ll keep searching, but nice article. Surprised I missed it when it came out.