Opioid overdose-related deaths have unfortunately been increasing over the last few decades, with the COVID-19 pandemic exacerbating this public health crisis even further. As a result, many scientists, healthcare professionals, and government officials have been working tirelessly to end this deadly epidemic. Researchers at the University of Washington are one such group and have recently unveiled a wearable to both detect opioid overdose and deliver an antidote, in real-time, restoring normal bodily function.
As the researchers describe in their paper, opioid overdose causes respiratory rate depression which will lead to hypoxia (insufficient oxygen in the blood) and ultimately death. Fortunately, opioid overdose can be readily reversed using naloxone, a compound that binds to receptors in the brain, outcompeting the opiates themselves, and restoring normal breathing. Unfortunately, if someone is overdosing, they are unable to self-administer the antidote and with many opioid overdoses occurring when the victim is alone (51.8%), it is necessary to develop an automated system to deliver the antidote when an overdose is detected.
The researchers begin by describing their process for measuring respiration, of which there are several options. You could use photoplethysmography in much of the same way we measure heart rate. Or you could measure the changing impedance of the chest cavity during breathing or even use an intraoral sensor that measures airflow in the mouth. Instead, the researchers opt to measure respiration by attaching accelerometers to the patient’s abdomen and measuring the movement of the abdominal cavity during breathing. They admit their technique becomes problematic when the patient is not stationary, but argue that in the case of a drug overdose, the patient is likely to be immobilized and the device would be able to measure respiration with ease. They tested their device across dozens of healthy, human volunteers, and even some opiate users themselves, and showed their technique had good agreement with a reference respiratory belt placed around the volunteers’ chests.
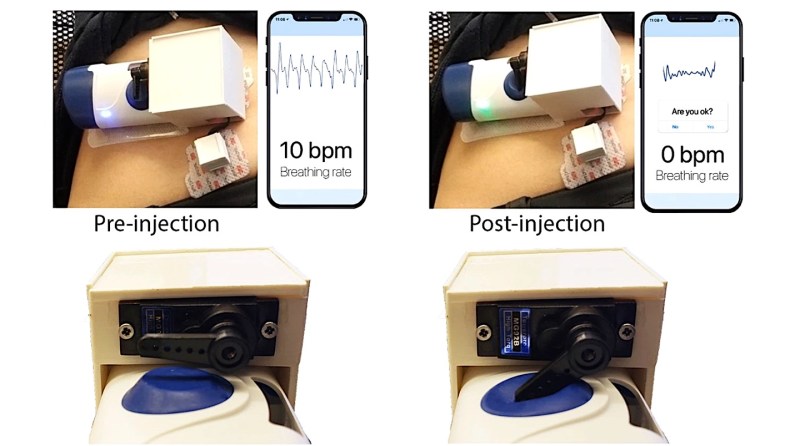
The cool part about this paper is that they demonstrated a “closed-loop” feedback system in which their device measured respiration, detected cessation in breathing (indicating an overdose), and delivered the antidote. To deliver naloxone, they leveraged an existing, commercially-available drug delivery system that requires a user to manually activate the device by pressing a button. They hacked the device a bit such that the trigger could be actuated using a servo motor properly positioned to depress the button when an opioid overdose is detected. They simulated an overdose by asking the healthy, human volunteers to hold their breath for a period greater than 15 seconds. They were able to successfully deliver the antidote to 100% of their volunteer group, indicating the device could potentially work in real-world settings.
Now, the form factor of the device undoubtedly needs to improve in order to deploy this device into the field, but we imagine those are improvements are underway and patients have shown willingness to wear such devices already. Also, there’s still a bit of a question of whether or not accelerometer-based breathing detection is optimal since some drug overdoses cause seizures. Nevertheless, this is an important step in combating the alarming rise in opioid overdose-related deaths and we hope to see many more advances in patient monitoring technologies in this field.














Are you Serious?
I mean, from OUR point of view this sound great…. BUT…..
But I worked as a volunteer for the Acid Rescue and Underground Switchboard Suicide and Drug Aabuse telephone hotline 271-3123 trough ST. Mary’s Hosp Milw back in my teen years, and on into my 20’s while in USA,. Milw WI. The hosp supporting this provided a doc, Doctor Alan Reed, at each concert,
Pink Floyd PIGS concert MILW… found a woman giving birth on the baseball diamond….. got her to the docs….. went back to scan my assigned area…. but took a sweep back to monitor the birth….
PPL are stupid about drugs and their circumstances…. letting events of the day override common sense…. more volunteers are needed to provide emergency assistance because at such stressful times the responsible parties are disabled by their own short term events.
I worked 80+ concerts. I care about you all.
My works… resulted in my Dad hating me. But it was a good tradeoff despite what Dad thought. Mom understood,. She was a Registered Nurse.
“Pink Floyd PIGS concert MILW…” – What?
“found a woman giving birth on the baseball diamond” – How is this incident related to the article?
“took a sweep back to monitor the birth….” – Who took what?
“My works… resulted in my Dad hating me.” – Why?
Use less ellipsis and more words to describe your meaning. Don’t get me wrong, I want to know what you are saying but you need to improve how your communicate.
What point are you trying to make?
Drugs are bad, mmm kay.
@Biomed: how true.
To quote TFA “… many opioid overdoses occurring when the victim is alone (51.8%)”.
Perhaps that’s the underlying problem. Perhaps the victims would resort less to opioids if they were “less alone” in the first place.
I mean: Im’ in for every gadget capable of saving lives (or even making them more brarable). But we tech geeks should keep some broader vision of the problem space. Especially when our PHBs tell us not to.
Being alone is not a problem perse. People constantly telling you that you are incomplete when you are is.
I disagree. Humans are social creatures, just like wolves, and various other animals. It’s not just a cultural thing. I’m sure there are people out there who can thrive in isolation, but most people can not.
One behavior us addicts exhibit is doing our drug of choice alone. Sure, we may do it with other people around too, but almost all of us will also do it without anyone around and without anyone knowing.
Addiction physically changes structures in the brain.
Thanks for sharing this.
I hadn’t really though about it, but I too prefer to do drugs alone. Upon reflection, I believe it’s because of the unpredictable nature of people. Others might react/behave differently to the drug, which might cause me to not be able to enjoy the high as much as I can when I’m alone.
When people get that far into their addiction, they will often withdraw from their friends and family. They get high or drunk or whatever by themselves and that’s when ODs are most fatal.
Having gone through treatment myself, I know this first hand and vicariously through counselors and other recovering addicts.
This could be a great help for harm reduction.
It won’t be because the people that need this are addicts that already use all their money getting the drug. Long-term strategies are not in the addict’s wheelhouse.
You believe Tom Petty lacked the funds? Addicts are not necessarily homeless needle junkies. Most addicts got the habit prescribed by a medical doctor.
Not all countries lack universal healthcare.
Are you kidding me?
Why on earth would you want to make it easier and “safer” for people to do these horrible, life-destroying drugs? This is only going to create more drug addicts. Take this down, hackaday, youa re disgusting. Do not encourage this. For pete’s sake. Shame on you.
Found the poster that doesn’t understand addiction.
Unless the so called victim was made to take opioids by force, it was voluntary. In this day and age, “not knowing” is a piss poor excuse, literally anyone in the 1st wold countries can just ask the greatest information service ever invented – the Internet – about the dangers of opioids. Just how bad can the addiction get. How easy it is to get addicted. That it will destroy, possibly even kill you. Where to go to have it treated. It’s all there, but…ignorance is bliss.
While I do support decriminalization of some substances based on their actual impact, opioids are not among them, along with meth. Those are proven many times over on how destructive they are to society.
Opioids are legal and have always been in most countries in the western world. When your physician prescribe pain killers for your whiplash damage, do you consider that a voluntary start on a life long addiction?
The proportion of opioid addicts who started on legally proscribed drugs is very small. (At least in the U.K.; if it’s different in the states you need to sort out your medical system because there shouldn’t be significant number of people getting addicted via medical channels).
But I question how useful this device is for them – the addiction is too powerful for them to ensure this device is set up properly. If there’s resources to get these distributed and used properly, let’s use that manpower to get people the help they need to get off drugs. A device like this would need to function reliably for months with no maintenance or adjustment and no battery replacement. And to take the abuse of a life on the streets.
You might manage to get some traction with the folks who come in for methadone – getting the pharmacist to check it’s set up properly – but I think most addicts don’t really care that much by that point.
Fundamentally, this isn’t solving the problem. Addicts dying of overdoses isn’t the problem. The problem is whatever caused them to end up on drugs.
In the USA, there is a huge “moral” argument that people shouldn’t be exposed to drugs or even told what drugs do. “Don’t tell kids about the good and bad things opioids do, that might make them addicts!” is not an uncommon expression.
If kids do use the internet to “do their own research” they end up with tiktok, facebook, and the like “learning” the pattern and exposing them to even more drug media. Sure, places like Erowid talk good and bad. But kids aren’t great at risk/reward balancing.
As a kid who had several surgeries before I turned 10, I was exposed to lots of pain meds, sedatives both benzo and barbiturates, and a lot more. I knew what they felt like, I knew both the good and the bad feelings they could bring. Friends would ask about them, but when the school did a “drug awareness” thing, no one was allowed to talk; I couldn’t even say aloud “nah, that med sucks because . . . ”
The puritanical system in the USA helps create the worst effects of addiction. Harm reduction and education could reduce deaths, but “addicts must be punished” and similar mindsets make the problems worse, not better.
Not everyone is affluent or aware as you or I. Take a trip to the city, it’s quite eye opening. Lots of people start taking drugs because they are very dissatisfied with their lives or they fall into a pit of despair. It’s a way of killing’s oneself very slowly, in some respects.
Harm reduction would be discussing ROA, effects, safety issues and ultimately trying to keep people from doing these drugs in the first place. I was vaguely active in the drug sub-community in this larger community I was apart & read Erowid (out of curiosity) before I did some very stupid (TM) things – so I was already well aware of the dangers and how to be safe. Even then, I had two accidents. First required some minor surgery. After the second, pure willpower allowed me to quit. People around me didn’t understand and took it personally, disowned me. Not very nice or Christian-like as they had claimed to be.
Now if quitting cigarettes was as easy… but I have a decent vaping system for cessation. Waiting for next delivery of liquids.
But yeah, recreational drug use or drug abuse isn’t going to help you solve your problems. It’s going to numb you up and delay one from addressing the problems in their life that are making them miserable in the first place.
Be safe, everyone and please be compassionate & understanding to your friends.
I think it’s fine that you don’t agree with the concept of harm reduction, but is it really offensive to you that other people believe in that strategy?
Something like this would only come into play once someone is deeply addicted, so I don’t see how it would result in more drug abuse. I will concede that other harm reduction strategies may be more of a double edged sword.
Primary harm reduction probably falls into understanding the pharmocology of the chemicals in question, the side effects, routes of administration, and reasons to not go ahead and do these things. If one is going to do them, primary harm reduction would be having a sitter for hallucinogens or perhaps even opioids. Making sure the user has naloxone if they’re going to do opioids or an SSRI or tricyclic anti-depressant to stop the effects of a bad trip (the pharmacology behind these drug interactions is facsinating).
I think a device like this falls under secondary harm prevention, just as police departments having nasal spray Naloxone kits to save someone from an accident or batch of heroin that has been stepped on and has way more fentanyl in it than actual heroin.
Personally, I don’t believe in places in say California that are personal places for people to shoot up drugs but rather I’d the money be spent on educating the masses on how this stuff won’t help your difficulties, they’ll just make it harder and waste a significant chunk of one’s life finding that out personally.
Only thing disgusting here is the call for censorship because you’re offended by a post.
Get a grip on yourself. Hysterics are how animals react.
Unfortunately some people will use opiates when they are alone and it is better to have at least some kind of safety solution for them. I agree that this should not be the primary solution for the opioid epidemic, however, this device in the meantime could help people to survive an overdose.
Looking at this with machine learning glasses on: Will this device train people to use the quantity of opioid at which this device kicks in?
I believe the current issue would be the erratic potencies street drugs have along with lacing them with God only knows what that can kill you.
No way. Aside from overdoses being unpleasant business, naloxone (Narcan) causes you to feel withdraw symptoms.
I’ve been told that getting hit with narcan is intensely unpleasant (due to almost instant crash from a high). Based on that I can’t see anyone triggering this intentionally.
Now I won’t claim to know much about drug addiction, but I suspect that the majority of overdoses are unintentional, and due to either carelessness, or inconsistent potency. I doubt it’s often a case of the addict taking an accurate dose that is slightly too high.
Where I am from, a majority of the crime in my area, including murder, robbery, sexual assault, and other violent and nonviolent crimes are committed by opioid addicts.
This is the case virtually anywhere that the opioid addiction is a problem in the local population.
And yet there are people commenting here trying to justify “addiction” as if the pills put themsevles in the addicts mouth.
“Oh, but my doctor prescribed them to me, they must be OK!”. Ever hear of thinkins for yourself?
You can not justify any addiction. Having an addiction problem is a personal problem which can only be overcome by the addict themself, there are countless examples of this, and there are countless people who have recovered, and some of these people give inspirational speeches at recovery groups, etc.
Please do not try to justify any addiction. That is ridiculous. Please do not try to justify any action as the result of an addiction, you are responsible for your actions, your addiction is not. This is the simple concept of personal responsibility that you must learn in order to become a real adult.
It is very sad that someone has created this device to make people “feel safer” doing their deadly, addictive drugs. What a sad state this world is in.
Waste of time and resources. Ask sc Johnson the family company who is #1 manufacturer of these chemicals how they magically lose track of a million pills a day. Bad choices lead to death and a better world for those who make better choices.
Saving people’s lives is a waste of resources?
Wow.
I guess you are an anti-vaxxer as well?