A pacemaker is implanted to send signals that regulate a patient’s heartbeat, and to do that, you need power. That means they require battery changes, and when the device in question happens to be inside your chest, that means surgery. Sometimes as often as every five years. [Alex Music] writing in Spectrum notes that researchers have a new paper discussing a possible alternative: a tiny patch stuck to the outside of the chest that uses ultrasound to pace the heart rhythm.
Rats, pigs, and human heart cell samples have all responded to the system. You might wonder how ultrasound could make your heart beat, but the new pacemaker relies on gene therapy to sensitize your heart cells to the high-frequency waves. The therapy is delivered by a simple injection.
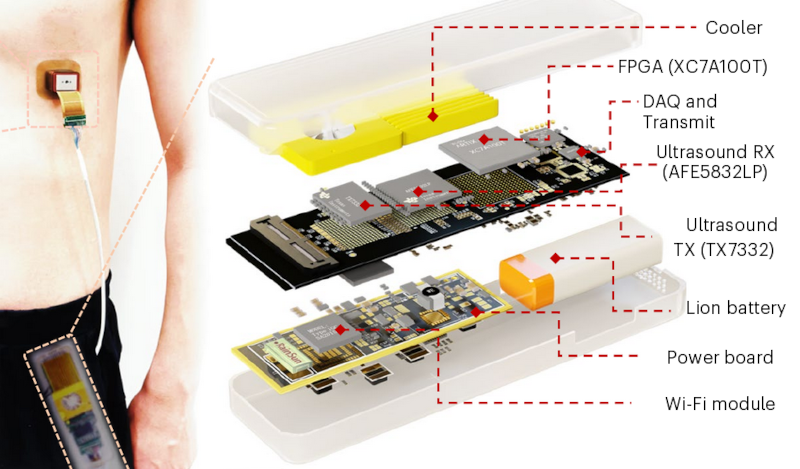
In addition to the chest patch, the patient would need a data and power module that they could keep in their pocket. The gene therapy doesn’t alter your DNA but introduces RNA to make heart cells produce a sound-sensitive protein in the cell’s ion channels. When stimulated, the ion channels admit calcium, which causes the heart to beat.
Pacemakers are nothing less than a modern technological marvel. Maybe if this catches on, cheap junked pacemakers will show up on the surplus market. They could be useful.













I’m a real doctor. This fever dream of what-ifs is damaging.
I don’t even want to elaborate but a battery change under local anesthesia every 5-10 years seems a reasonable compromise for.. living.
Idunno, contemplating what-ifs seems pretty important to the scientific method and advancement of technology.
I’m a physician scientist. Saying we have an idea for transcutaneous pacing but that won’t work so we’re gonna modify your genetic makeup or RNA. Yeah that’s it. Then it will all work!
That’s not how medical science works. That’s how nonsense investor fishing ad copy works and how it damages science is because it doesn’t even pass the sniff test for the general public and then we all look untrustworthy. The public thinks “yeah these people are full of it” and they are right.
I’m a layman Craig. Could you explain why the idea doesn’t pass the sniff test? What’s wrong with this idea?
It’s often, if we do this, we reduce or eliminate this risk or effect, but of course there are newly introduced risks. An external pacemaker will probably have a greater risk of losing signal contact with the heart compared to an internal device. But there probably will be situations where this is beneficial to the patient; so for me this is still very interesting research. That doesn’t take away that current pacemakers are incredibly useful and a wonder of technology, and of course all respect for the people connecting these devices to beating hearts.
Patient dies due to unexpected frequencies in the latest hit single. Rhythm nation hard drive crashes all over again, but heart muscle.
Human hearts have been insensitive to sound waves for about 300 million years. Suddenly raising this sensitivity in an environment where it’s never been an issue is a recipe for disaster.
Pretty sure they wouldn’t use anything your hit single is likely to reach. Now maybe if you were swimming next to a navy sub…
Agreed. Surgery sounds bad, but this could be no more tricky than some piercings.
That said, replacing a leadless pacemaker is dramatically more work and this has even more benefits than a leadless.
Let’s take the frail patient, perhaps with cognitive issues where a leadless would be ideal to avoid repeat procedures over the life expectancy, benefits from not risking rotation or rotation/displacement by the confused patient.
But has the risk that the surgery itself. What if they are not fit for surgery? Have had endocarditis? Or ongoing infection? This seems quite ideal for the next week’s to months.
Slap a sticker on the person is excellent outcome for that group.
My concern is the gene therapy to sensitive the myocardium, how likely is it that this is desirable unless the pacing is purely to overcome heartblock with a brady escape rhythm?
Are they going to have commotio cordis from a cough?
Article is definitely HAD worthy. Even if I can’t see it in use.
My fear with something like this is the inevitable “DRM” whoever brings it to market will impose. EG the specific freq of the ultrasound, timing params, etc, patent on the process. Will people drop dead because they can’t afford their new proprietary pacemaker?
Yeah, but a frail person receiving a viral vector gene therapy? I’m not sure that works anyway?
Regardless the article’s actually really impressive. Including the actual layout of the board was a surprise.
Unsure if you are aware but a leadless pacemaker is already a widely used thing. It’s is a small device implanted/anchored into the atrium via a catheter usually through a groin vein. They can and usually are placed with light sedation and avoid general anestheisa all together. Replacing one… does not happen. They just place a new one and leave the old one there.
A couple hundred years ago surgeons said “Pain can never be separated from the knife.” and today we do organ transplants regularly. The what-ifs of today may become the commons of tomorrow, let’s see where this leads. You have to agree that surgery every 5 years isn’t bad but surgery never for the same benefit is better?
It’s not surgery. Changing a device (even placing them) can be very well tolerated by even the sickest patients …and also not. It is a needle poke and a 3cm skin incision. All can be done with simple skin infiltration of local anesthetic. You need a good doc though I’m not denying that.
.
A couple hundred years ago opium and morphine were well known. Chloroform was well known in the US civil war despite the widespread beliefs.
.
We still cannot separate pain from the knife. That’s why there are board certified anesthesiologists and pain medicine physicians that specialize in this.
We already have transcutaneous pacing. Allll the time. Requires basically deep sedation in the ICU to even be tolerated. The physics of applying a couple tens to hundreds of milliamps through the chest wall will not change. It is extremely painful. They are used in sedated ICU as a bridge to a proper pacemaker or more commonly an AICD.
.
All I’m saying is I’m not perfect or whatever but I’m very, personally involved in this topic fairly for the last 20 years. And this is dumb. Take it or leave it.
How do they maintain pacing during a device replacement for a fully pacemaker dependent patient (i.e. total AV node ablation, no escape beats, no device=no life)?
Is it fast enough that they just let the heart stop for the time the leads are unplugged?
The EMTs carry equipment in their bags that when I was a kid you could only find at the hospital. I am not going to worry too much about blue-skying new equipment because when it works out it is a game changer. This is the sort of thing that might help compensate for a patient who doesn’t need a pacemaker or an ablation, but the pills aren’t helping the tachycardia enough.
There is so much faffing around before they decide to do anything on the heart, that if they could do a couple of shots and a patch for a month it would be a benefit.
There is a big difference between “we have discovered new tech that works in the lab or in animal tests” and “we have something that is good enough to actually try on a real living human in a clinical trial”
I alwats thought that a clinical trial is the next step after both “works in the lab with human cells” and “tested on animals” have passed.
What is in between ?
The 3 phase clinical trials are next, then the approval review itself.
Surely inductive charging would be a more preferable solution than genetic modification. If you’re going to do that, you might as well take a leaf from those frogs that freeze solid in the Arctic or maybe electric eels and have the body produce an electric potential for itself.
It begs the question whether gene alterations, applied to brain cells, could influence the rhythm of certain functions. Breaking people out of depression on one hand, making people buy a certain product on another. Even worse still if the changes are passed to subsequent generations be them genetic or epigenetic changes.
It feels like a terrifying future. This is essentially a wild west with global implications.
“Even worse still if the changes are passed to subsequent generations”
This doesn’t affect the genome. It’s just giving new (RNA) instructions to heart cells.
If you’re targeting neurons or heart muscle or something it’s not going to end up modifying their genome. Especially those two since those cells are very long lived: shRNA for instance will stick around functionally for many many years but the DNA can’t be affected.
I am curious now why we don’t use inductive charging.
Perhaps it’s concern for the risk of a problem damaging the cell and causing the battery to explode inside.
Maybe rechargable cells aren’t as reliable or hold their charge over time as well as whatever cells they currently use.
Idk, without more info it seems like a LSD NiMH with Inductive charging should last a lifetime and not need frequent charging.
Rechargeable battery chemistry adds a whole lot of extra concerns like venting, overcharging, thermal runaway.
Because regular batteries are so well proven and changing the device is so easy. It’s done under local as outpatient procedure. And again. Low price to pay for being alive.
The devices themselves are getting so much better that by the time you need a battery change (years) the device itself is obsolete and you get the new way better one.
The tech in these things is incredible. I’ve been alive long enough to see the evolution from basically dumb devices that can barely change heart rate to extremely advanced ones with all the modern connectivity you’d expect and very advanced rate adjustments based on a whole bunch of parameters all measured in real time. Actually as an aside I’m very worried that some tech in an office in middle America can click some boxes and turn off an AICD anywhere in the world within WiFi range.
.
That’s what you all should really be talking about.
We can make stomas. Just put a USB-C port on their chest.
Probably want to use something less common than a USB in case anyone wants to either do a self-recharge or maybe hack it to run Doom.
I read the title and thought the pacemaker patch was going to be a patch as in “patch Tuesday”! Forgive me for being slightly disappointed!
The referenced article does a nice job of laying out the challenges to this technology.
Additionally:
There are multiple pacing modes and they are based on the underlying condition. Since this method sensitizes ALL of the heart muscles then you are limited to a single mode of pacing which is not going to be appropriate for many patients.
Leaving an adhesive patch on the same area of skin will eventually cause skin breakdown. Moving the patch could be troublesome as it might affect the heart’s response and/or the device’s sensing.
The risks and long-term effects of genetically altering the cells of a damaged/diseased heart requires more research and vetting.
It’s an interesting concept, but I don’t see it being a viable alternative to a proven technology that allows many people to enjoy a fairly normal life.
Finally.
Thank you.
The original pacemakers solved this problem with a bit of radioactive material.
First thought… being external, what happens if it gets damaged?
Second thought… it can be ripped off and maybe that’s a good thing.
One horror story about pacemakers I have heard is what can happen when one is dying. The pacemaker keeps trying to shock the heart. It doesn’t save the patient but it does draw out the death process adding lots of painful shocks.
I’m pretty sure they figured that one out though and modern pacemakers have programming to detect this and stop themselves. I’m no expert in that. So back the first thought. What if it gets damaged when the patient wasn’t already in the process of actively dying?