As the many many warnings at the base of the Open Surgery website clearly state, doing your own surgery is a very bad idea. However, trying to build a surgery robot like Da Vinci to see if it can be done cheaply, is a great one.
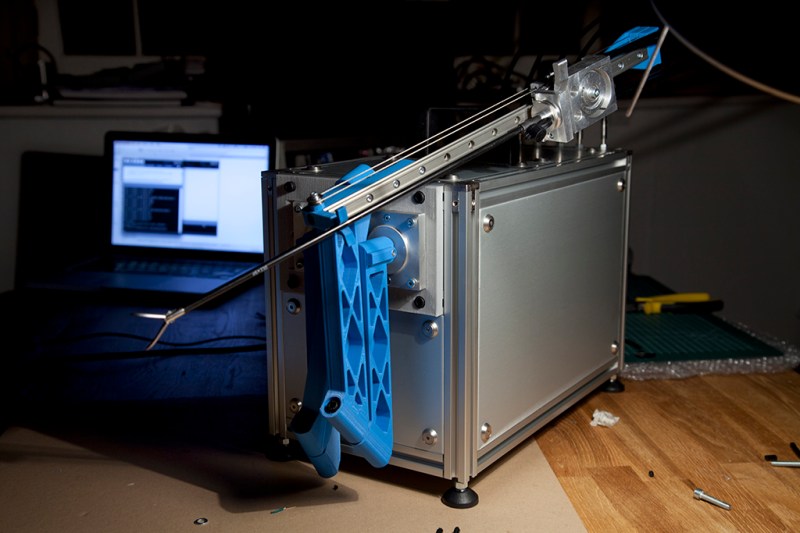
For purely academic reasons, [Frank Kolkman] decided to see if one could build a surgery robot for less than an Arab prince spends on their daily commuter vehicle. The answer is, more-or-less, yes. Now, would anyone want to trust their precious insides to a 3D printed robot with dubious precision? Definitely not.
The end effectors were easily purchased from a chinese seller. Forty bucks will get you a sterile robotic surgery gripper, scissor, or scalpel in neat sterile packaging. The brain of the robot is basically a 3D printer. An Arduino and a RAMPS board are the most economical way to drive a couple steppers.
The initial version of the robot proves that for around five grand it’s entirely possible to build a surgery robot. Whether or not it’s legal, safe, usable, etc. Those are all questions for another research project.













“Now, would anyone want to trust their precious insides to a 3D printed robot with dubious precision? Definitely not.”
I expect that, right now, there is at least one person in the world who would be just fine with a noob medical student using this device and a crappy webcam over the internet to do surgery on them, because it’s better than any other option they have available.
Very true, imminent death tends to change your priorities, but the chance of said person and machine ending up in the same place and having a data-link to the remote operator are another matter altogether. I’m guessing 1 in a few hundred million at best.
There are hordes of 18-35 year olds like myself with dubious medical coverage and a lack of employment opportunities that would be just fine with it.
Really, really, wanting to see Simone Giertz’s version of this one, more so than tattoo bot :-D
It’s okay she’s doing some stuff with Adam Savage, so he can prolly show her how to make ballistic gel dummies…. containing plenty of ketchup for realism…
Here ya go.
https://www.youtube.com/watch?v=EbmQxZkSswI
It’s entirely plausible that in a few years we could ship a couple of crates to a 3rd world aid station and perform complex surgery across the internet.
Technically that would have the same problems as building a clinic with a real Da-vinci robot…
This doesn’t magically do everything, somebody still has to clean and sterilize the tools, occasionally service the robot, clean the operating rooms and so on…This is what’s usually terribly lacking in the 3rd world countries, it’s not the surgery that kills most of those that do not survive, it’s the complications after it, infections being probably in the top 3 causes of death. No point in doing an 8 hour surgery for brain tumor if you know the patient has only a few % chance of survival because the place he’s being taken care of is an infested shithole.
This is very unlikely to reach the 3rd world, instead they are a prime candidate to be in remote places where 1st worlders live/work and can’t afford to keep an entire hospital at ready.
What’s nice about it is the size…maybe humanitarian effort missions for natural disasters and warzones would be a good start, they have money for the gear and some qualified medical personnel to make sure the patients can survive after the surgeries.
In reality, just another medical SKU the warlords can thieve in transit and deprive humanitarian disaster victims of.
The USA has several forms of healthcare, but essentially is 3rd world style services if you can’t afford private insurance.
Warlords tend to stabilize the anarchy of desperate peoples, usually have economic motivations, and enforce a bare minimum set of rules. These rules are generally unfair to the weak, but eventually evolve into a set of laws.
When society is able to function independent of authoritarian dictators – it will.
Dictators are a symptom of peoples’ inability to influence their own governance.
What people consider intelligent can actually be quite dangerous:
“The Basic Laws of Human Stupidity” ( http://www.extremistvector.com/content/stupid.html )
Open open heart surgery. ;P
(I’m sorry.)
:D but nope ! Those tools are used for Minimally-invasive surgery, so not open surgery !
I really like it. The technology have to spread to all the word eventually. And also this device doesn’t have to be perfect, just have better pulse than a human and smother movements. With some tunning and testing might work well to use in real surgery.
Also, forget about surgery over the internet in 3rd word countrys, they don’t even have a good connection to use skype so…
Repurpose it as a sushi robot. (No fugu.)
They don’t use Da Vinci surgical robot in Poland, first world country, because it’s too expensive both in materials and staff. Any decent surgical robot would have to be as capable as that machine to be useful, so no one would bother with it unless it will be cheaper than Da Vinci without compromising the safety of patient. And I wouldn’t trust anything that uses Arduino, RPi or other such thing to mess with my insides…
Arduino is basically just a microcontroller broken out to be easier to use– and the brains of a typical 3d printer is a cheaper version of an industrial controller in the first place. Reduce the cost of the moving parts enough and you have a much cheaper machine even with the same brain.
Arduino is not only a microcontroller, but entire ecosystem, including libraries, that aren’t optimized. If you are doing a safety-critical system, you don’t use Arduino. You use hand-optimized Assembly or bare C compiler. And you use medical-grade parts, not something made cheaply in China. I think Microchip has in some datasheets a disclaimer stating “This part is not rated for safety-critical systems”, and probably with good reason. Imagine that voltage fluctuation causes Arduino-controlled robot to glitch while it’s cutting the patient with scalpel, and before anyone could react, robot disembowels poor victim, who only had a mild case of appendicitis. What if one of Arduino libraries has hidden error that causes race condition to occur? That would be worse than Therac-25 accident…
Yeah–but for developing the hardware side that *can* be controlled by a proper brain, that’s fine. And it’s everything *but* the bits that actually go inside people that can be reduced in materials cost for the most part.
“Beware of bugs in the above code; I have only proved it correct, not tried it.”
The problem and hence solution lies not in identifying the right brand, library, … but in society adopting a new way of living: requiring publicly available proofs that anyone can verify in an automated fashion. A provable society.
You certainly don’t use hand-written assembly language in any half-complex, safety-critical system. Usually you use a reasonably high-level language that has available tools and processes for formal verification, as needed. You can do this with C++, but I also certainly wouldn’t go with the processing libraries for such a application, mainly for performance reasons, though. Also please note that a common 3D-printer driver as used here is better tested through sheer runtime than any medical device ever is before getting to market. See Therac-25.
Maybe surgery on animals? PETA might object but then explain that it’s only to be used on injured animals that would be unlikely to survive without it.
I can imagine people driving around looking for injured animals on roadways to save with a surgical robot.
I dunno… Hospitals can be really hazardous places, and there are a lot of careless and/or incompetent surgeons who might do you serious harm (happened to me once). I’m not sure that DIY surgery is ???????????????????????????????????????????? that much riskier.
How many forceps did we use?
10… 9…
Bah, probably dropped one on the floor.
I’m sure of it…
The way LINS has killed Ontario (–Canadian–) Heath Care this is the way we will be going. And no we cant goto another provence to have the surgery done. The canadain goverment wont let you.
AS it stands now you have a better chance of living if you can afford to go to another country and have the surgery done.
Because you will DIE WAITING here…… For Me I would take the chance here and build the robot my self, because I cant afford to goto another country and pay.
Good way to get your name out in the press, if nothing else.
In disaster situations the killer is usually not the complexity of the operations, but the huge numbers needed and the delay in bringing in doctors. A few of these tele-operating could do a world of good, the machines can run basically 24/7 while doctors work in shifts, possibly even by time zone. Similarly, while you wouldn’t want to drop one of these in the bush, a single specialized surgeon could service several remote clinics. One of the biggest problems in third world health care is the dispersed nature of care providers and the poor transportation infrastructure which leads to long delays in care. Lowering the price of equipment can increase the number of outlets and tele-medicine is a huge multiplier. I doubt any homebrew machines will ever see service but the open nature of the design may encourage new entrants into the field, thus driving costs down.
In the old movie *Silent Running* this deranged idea comes up. Bruce Dern (real life name of the actor) gets a robot to do a minor surgery job mid-flight. While not ready now, wait a while, we will be able to get that nose job done on a DIY basis. This, combined with skin color change will make racism obsolete.
I’m not entirely sure how that would work, unless A: Everyone wants to change their skin color/facial features, or B: Everyone is forced to undergo cosmetic surgery to look exactly the same. Surgery doesn’t change your genetics, either, so this would have to be undertaken from a very young age every time a child is born. None of that seems at all likely (in the case of A) or ethical (in the case of B). In the case of A, there would still end up being patterns to be prejudiced against, and in the latter case, people can still be bigoted even if there are no apparent physical differences.
Yeah but imagine, if you could pick your skin pigmentation, you could pick chlorophyll and save $$$$$$$$$ on food.
Enjoy not having any protein or vitamins …
https://en.m.wikipedia.org/wiki/Leonid_Rogozov