Blood pressure is one of the so-called “vital signs” that medical practitioners use to determine the basic state of a patient in any given moment. It’s exactly what it sounds like—a measurement of the pressure of the blood flowing through the body, with some complications to account for the pulsatile nature of human blood flow.
You might think measuring blood pressure is a solved concern, and it mostly is. With that said, some blood pressure monitors out there aren’t quite doing their job properly, and [Milos Rasic] came to Hackaday Europe 2026 to spell out the problem.
Under Pressure
Before exploring the issue, it’s worth first understanding how blood pressure is actually measured. On a baseline level, it’s the same as pressure being measured in any other fluid. Specifically, though, when it comes to blood, it’s important to measure the pressure at two points. There is the peak, when the heart muscle is contracting, referred to as systolic pressure, and the low point, when the heart relaxes, referred to as diastolic pressure. Thus, blood pressure is referred to with two numbers, such as “140 over 90” or 140/90, referring to systolic and diastolic pressures respectively. It’s sometimes important to track the mean arterial pressure, too. Typically, nominal blood pressure would be considered around 120/80 mmHg. High blood pressure, or hypertension, starts at figures over 130/80 mmHg, while low blood pressure, or hypotension, would be considered relevant below 90/60 mmHg.
Blood pressure can be monitored in a number of ways. Most of the time, non-invasive methods are preferred, whether in the doctor’s office or at home. [Milos] notes that the classic hand-pumped blood pressure cuff device (sphygmomanometer) and a stethoscope is still a perfectly excellent way to measure blood pressure in a clinical scenario. This is referred to as the Korotkoff method, where the doctor listens for pulsations in the artery to begin as the pressure of the cuff slowly drops below the systolic pressure, and then later ease as it reduces below the diastolic pressure, monitoring pressure in the cuff on a gauge as they go. Then there are digital versions of arm cuff blood pressure monitors, which [Milos] notes can have some problems. Meanwhile, there are advanced technologies in development to do live measurement with things like mmWave radar devices or ultrasonic tricks, but they’re still emerging and less established in clinical contexts.
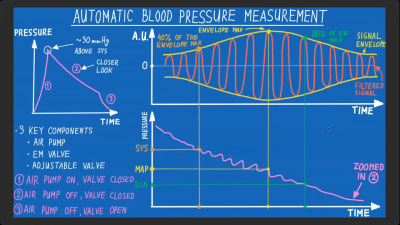
Many cheap electronic blood pressure monitors use the oscillometric method to measure blood pressure. Few manufacturers share the algorithms they use, but [Milos] has found many use something similar to the above, approximating systolic and diastolic pressures from measurements taken to find the mean arterial pressure. Credit: presentation slides[Milos’s] talk focuses on the digital oscillometric analysis that is behind cheap electronic blood pressure monitors that commonly retail for $30-50. These devices start by pumping up an arm cuff to well above typical systolic pressures, before slowly letting it deflate. A sensor hooked up to the cuff is used to monitor the pressure during deflation. When the cuff is below systolic pressure but above diastolic pressure, the pressure in the cuff will oscillate with the pulsing of the blood flow. When isolated from the overall pressure loss from deflation, the amplitude of this oscillatory signal is maximum at the mean arterial pressure. According to [Milos], it’s common for electronic blood pressure monitors to then take some figure like 40% and 80% of the amplitude of the oscillation envelope, and grab the systolic and diastolic pressure values at those points. As far as accuracy goes, this method isn’t exactly perfect, being more of a useful approximation rather than something that’s rooted in a true direct measurement. Furthermore, [Milos] notes that, for example, Category A blood pressure monitors are only expected to land within a +/- 15 mmHg range, for 85% of their measurements. That’s not fantastic.
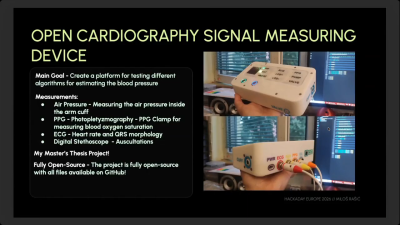
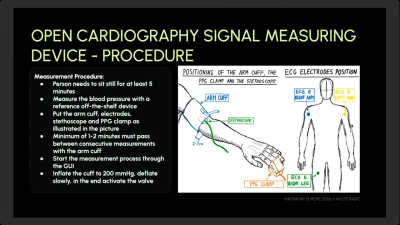
[Milos] has invested a great deal of time into the Open Cardiography Digital Measuring Device, hoping to better investigate alternative methods of measuring blood pressure in a non-invasive manner.[Milos] notes that it’s important to allow the patient to sit still for five minutes before measurement if numbers are to be at all comparable between checks, as many factors can influence blood pressure in the moment.The method used by these electronic devices tends to be a little inaccurate compared to the traditional clinical methods performed by trained professionals. For that reason, [Milos] developed the Open Cardiography Signal Measuring Device. It is specifically designed to test different algorithms for blood pressure measurement. It can measure pressure in an arm cuff, and also takes signals from a photopletyzmography (PPG) clamp for measuring blood oxygen saturation. There are also inputs for ECG and digital stethoscope signals, too. [Milos] has published the device’s design on Github for anyone to explore as desired. His talk explains how the device came together, and how he has been using it to evaluate the accuracy of off-the-shelf monitors and the use of alternative algorithms to those used in such units. He also discusses the challenges of measuring blood pressure accurately in this way when dealing with, for example, patients with less stable heart rates.
It’s an interesting exploration of a very specific part of vital sign measurement that few of us ever think about in detail. Sometimes it pays to know how the machines that you’re getting measurements from actually work, and whether you can trust what they’re saying. In the world of blood pressure measurement, [Milos] has done just that.
21 thoughts on “Hackaday Europe 2026: Is Your Blood Pressure Monitor Lying To You?”
A lot of the cheap smart/sport watches simply give you random numbers to pretend they’re measuring your blood pressure. They can’t even detect when the watch is placed on a table instead of on your wrist. If it doesn’t even check for a pulse and throw an error, that’s a dead giveaway.
I’ve seen a few ads for smartphone apps that claim to work as a diabetic glucose meter, without adding any hardware. These seem to go past selling unapproved medical devices into reckless endangerment.
The cheapest Chinese ones (10$ and below) are legitimately just step counters. They might appear to have heart rate or SPO2 sensing but more often than not, it’s just a singular red/green LED present, but there’s no sensor or phototransistor to actually capture the information. The LED is purely there to mislead people
The however do have functional BLE. I think that’s a testament to how cheap ble microcontrollers have become at least in China. A shame, us engineers in the West who can’t read Chinese cannot benefit though
There is a bunch of papers about measuring BP from e.g. two PPGs or PPG+EKG and it all boils down to predicting mean for given population combined with estimating whether is the person currently active or e.g. sleeping.
I.e. guesswork or outright lies. Also, they usually contaminate results by training on say 10s windows and splitting training/testing data as 80:20 but from the same subjects.
There is an actual, relative arterial stiffness signal (PTT – EKG/PPG lag, PPT – systolic to diastolic PPG peak lag) and these are real and useful, but absolute mmHg are just not possible using these non-invasive methods, period.
Making the person sit still for 5 minutes, and asking them to relax is very important. Any emotional stress or recent physical activity (something as minor as climbing a flight of stairs) can increase the BP by 20/10. This is highly important
Doctors don’t think twice before prescribing BP meds to patients. Some patients do require them but most simply need to relax and reduce the amount of caffeine, alcohol and salt in their diets. The problem with BP meds is that they introduce an entirely new variable into a natural control system loop. Anyone who has taken control systems 101 knows the issue, you’re disturbing a control loop, it may just go out of control.
I have a family history of hypertension but turns out if I control my diet, basically eliminate caffeine and reduce salt, I can remain in the healthy BP range without having to take any pills.
Just like [Milos] I take care of my grandparents. At a certain age, human bodies get worse at regulating BP (cold can increase BP, warmth can decrease BP by making you sweat and losing salt) naturally, hence medicines are necessary at that point
THIS!!! Everywhere I go from the dermatologist to the dentist seems insistent on taking my blood pressure incorrectly for no other reason at all than to have something to chide you about. “Hmm it is a little high…” YEAH because you surprised me by calling my name in the waiting room I dont want to be in for a malady I may or may not have, and had to battle traffic to get to. You then lead me on a quarter mile maze to my room and then immediately sit me down to take my blood pressure, audibly snorting in lazy disgust of the task the entire way! Of course it is gonna be higher than normal. Hilariously if my SO is in the room, I shoot 20 points lower on average lol.
What shinsukke said about age and medication is also true. The body wears out over time. I recall my mom was having all kinds of BP regulation issues and of course was overexercising and avoiding all foods etc. In the end a simple pill and some water fixed all that but really she was killing herself in other ways just to get some numbers settled at the cost of other body systems.
Now I just say no or tell them not to ask about the BP cuff in the future. It raises my blood pressure to know I will have to battle them about it lol.
As far as the article that is super true. Most of the watches and such just use an algorithm on the pulse and o2 from what I have seen. They are what they are. If I believe my watch I levitate from my bed 40-200′ about twice per week lol, so that is where I hang my hat. Good to have an idea and watch out for patterns that may mean something but also it is a dumb computer with sensors that have to survive normal human life and thusly may be not as accurate. The cuff things aren’t usually too far off but that is specialized hardware.
Interesting story – last time I went to the dentist they took my blood pressure. At the time it was quite high and they said they couldn’t use the standard stuff to numb my mouth before drilling because apparently in addition to the numbing agent there’s a vasoconstrictor to keep the numbing agent from getting washed away too quickly.
So they had to use a different kind of numbing agent which only lasted about 5 minutes before feeling came back. Needless to say it was painful not only when drilling but also when re-applying the numbing agent.
Thankfully my doctor ignores the blood pressure measured by their MA/CNA and checks it himself right before my visit is over. A 15 minute wait is the difference between “high” BP and just average for me.
Useless dentist and ignorant too.
Bupivicain on its own will five at least four hours numbness and lidocaine gives about an hour.
There are others with similar durations. (I use the agents in my anesthetic practice.)
The added adrenalin in the locals will increase the time but unless the toothpuller is a tortoise it’s really not needed.
Change your dentist.
One of the main effects of getting older is that the elasticity of the arterial vessels reduces, as they become stiffer (and probably, calcified, in most westerners particularly). This means that their elastic recoil isn’t as able to absorb the sudden increase in arterial pressure that comes with systole.
Also, organs will start, over time, to adjust their autoregulation abilities, so they become accustomed to running with higher blood pressures, and will then misbehave when the pressure drops.
Congrats on being the one person in a thousand willing to take medical advice and look after themselves. Everyone else just wants a pill, and to take no personal responsibility for their health, especially if they have to give up anything they like. (I’m in the 999 myself, but hopefully one day I’ll change (though probably too late).)
White coat syndrome is a real phenomena too, perhaps as high as 1/3 of patients. Just getting your blood pressure taken in a doctor’s office makes it high enough to result in a misdiagnosis. Conversely home based monitoring can trigger hypochondria. Then there is the direct impact of pain on BP results. Actually getting good well normalised data for BP over time takes more than accurate technology.
There is an additional way it can be done in critical care departments and is hinted at in the text above. ‘Invasive’ monitoring – where a plastic cannula tube is inserted into an artery (wrist, elbow, groin, usually), and attached to a pressurised bag of fliud and a transducer. The transducer is zero’d at atmospheric pressure, and will then record the peak (systolic) and trough (diastolic) pressures on a beat-to-beat basis. It’ll also give you a continuous waveform of the pressure changes with each heartbeat.
It has a couple of other advantages – being beat to beat, it’ll react immediately if there’s a problem, and also you can infer several things (about myocardial contractility and vascular resistance) based on the waveform itself.
There is no requirement for testing and calibration of these in doctor’s offices, in Canada at least.
The tubing and cuff can leak, sensor shift etc. They don’t last forever.
Caused me great trouble because my GP’s reads at least 30mmHg low. Found out the hard way at other clinics freaking about hypertension. The company making the (really good actually) product went out of business almost 10 years ago. So GP’s got old units.
At home, the Omrons are terribly inconsistent, but they blame it on your body. Not the crappy tech Omron has. Never the same reading, drives me nuts. Am I dying or not.
This has been said, but is worth repeating: If you don’t consistently sit quietly and relax for five minutes, the readings will likely trend high, probably by quite a bit more than any inaccuracy of a halfway decent instrument.
Maxim makes an optical chip that can take BP. Not (not!) easy to program. But it does a pretty good job on at least some skin types. You need to have a bone behind the skin for reasonable readings (wrist, forehead).
I put it into a device about 4-5 years ago. It really does work.
I worked for a company who made, amongst other devices, a blood pressure measurement device. It was of the inflatable cuff type, and had quite a good dsp and algorithms inside to do the work, not like the cheap $30 devices. The device underwent clinical trials and the measurements were very good, corresponding quite good to what the doctor would read when doing a manual blood pressure measurement. Of course, provided that the patient would keep to the instructions. All very interesting work.
Sadly, the company went bankrupt because of some short seller investment group targeted our company’s main investor, and our main investor pulled out their investments because they got into a whole lot of trouble and got cold feet. The short seller made a few million dollars, and at least 5 startup healthcare companies went bankrupt. And people wonder why healthcare is unaffordable…
Anyway. It would have been nice to use Milos’ knowledge to see how close we were to the ideal, and if we could get any closer.
I think the electronic devices are infinitely better than taking the reading manually, for 1 reason. They use documented algorithm and do it the same way every time. I’ve watched nurses take me and my wifes blood pressures many times, and despite the seriousness of it, they almost always half ass it. They throw that cuff on over clothing, don’t bother with body positioning, and they drop the pressure in only a few seconds. If her heart is beating at 60bpm, how many mmHg is the needed dropping between heartbeats? Quite a few. I’m sure it’s possible to get an excellent reading manually, but I don’t think I’ve ever seen a nurse attempt it.
I love how complex terms like:
systolic pressure and diastolic pressure
are used in medicine. The big number (systolic) is the maximum pressure (in mm of mercury ; ~16 kilopascalsl ;~2.3 PSI) inside your arteries as your heart pumps out blood (while resting). And the smaller number is the pressure inside your arteries between the beats of your heart (~10 kilopascals ; ~1.5 PSI).
They are basically a measurement of how hard your heart has to work while idle. If your arteries are coated with a layer of fat the amount of work that your heart needs to do increases.













A lot of the cheap smart/sport watches simply give you random numbers to pretend they’re measuring your blood pressure. They can’t even detect when the watch is placed on a table instead of on your wrist. If it doesn’t even check for a pulse and throw an error, that’s a dead giveaway.
I’ve seen a few ads for smartphone apps that claim to work as a diabetic glucose meter, without adding any hardware. These seem to go past selling unapproved medical devices into reckless endangerment.
The cheapest Chinese ones (10$ and below) are legitimately just step counters. They might appear to have heart rate or SPO2 sensing but more often than not, it’s just a singular red/green LED present, but there’s no sensor or phototransistor to actually capture the information. The LED is purely there to mislead people
The however do have functional BLE. I think that’s a testament to how cheap ble microcontrollers have become at least in China. A shame, us engineers in the West who can’t read Chinese cannot benefit though
There is a bunch of papers about measuring BP from e.g. two PPGs or PPG+EKG and it all boils down to predicting mean for given population combined with estimating whether is the person currently active or e.g. sleeping.
I.e. guesswork or outright lies. Also, they usually contaminate results by training on say 10s windows and splitting training/testing data as 80:20 but from the same subjects.
There is an actual, relative arterial stiffness signal (PTT – EKG/PPG lag, PPT – systolic to diastolic PPG peak lag) and these are real and useful, but absolute mmHg are just not possible using these non-invasive methods, period.
Making the person sit still for 5 minutes, and asking them to relax is very important. Any emotional stress or recent physical activity (something as minor as climbing a flight of stairs) can increase the BP by 20/10. This is highly important
Doctors don’t think twice before prescribing BP meds to patients. Some patients do require them but most simply need to relax and reduce the amount of caffeine, alcohol and salt in their diets. The problem with BP meds is that they introduce an entirely new variable into a natural control system loop. Anyone who has taken control systems 101 knows the issue, you’re disturbing a control loop, it may just go out of control.
I have a family history of hypertension but turns out if I control my diet, basically eliminate caffeine and reduce salt, I can remain in the healthy BP range without having to take any pills.
Just like [Milos] I take care of my grandparents. At a certain age, human bodies get worse at regulating BP (cold can increase BP, warmth can decrease BP by making you sweat and losing salt) naturally, hence medicines are necessary at that point
THIS!!! Everywhere I go from the dermatologist to the dentist seems insistent on taking my blood pressure incorrectly for no other reason at all than to have something to chide you about. “Hmm it is a little high…” YEAH because you surprised me by calling my name in the waiting room I dont want to be in for a malady I may or may not have, and had to battle traffic to get to. You then lead me on a quarter mile maze to my room and then immediately sit me down to take my blood pressure, audibly snorting in lazy disgust of the task the entire way! Of course it is gonna be higher than normal. Hilariously if my SO is in the room, I shoot 20 points lower on average lol.
What shinsukke said about age and medication is also true. The body wears out over time. I recall my mom was having all kinds of BP regulation issues and of course was overexercising and avoiding all foods etc. In the end a simple pill and some water fixed all that but really she was killing herself in other ways just to get some numbers settled at the cost of other body systems.
Now I just say no or tell them not to ask about the BP cuff in the future. It raises my blood pressure to know I will have to battle them about it lol.
As far as the article that is super true. Most of the watches and such just use an algorithm on the pulse and o2 from what I have seen. They are what they are. If I believe my watch I levitate from my bed 40-200′ about twice per week lol, so that is where I hang my hat. Good to have an idea and watch out for patterns that may mean something but also it is a dumb computer with sensors that have to survive normal human life and thusly may be not as accurate. The cuff things aren’t usually too far off but that is specialized hardware.
Interesting story – last time I went to the dentist they took my blood pressure. At the time it was quite high and they said they couldn’t use the standard stuff to numb my mouth before drilling because apparently in addition to the numbing agent there’s a vasoconstrictor to keep the numbing agent from getting washed away too quickly.
So they had to use a different kind of numbing agent which only lasted about 5 minutes before feeling came back. Needless to say it was painful not only when drilling but also when re-applying the numbing agent.
Hydralazine.
Thankfully my doctor ignores the blood pressure measured by their MA/CNA and checks it himself right before my visit is over. A 15 minute wait is the difference between “high” BP and just average for me.
Useless dentist and ignorant too.
Bupivicain on its own will five at least four hours numbness and lidocaine gives about an hour.
There are others with similar durations. (I use the agents in my anesthetic practice.)
The added adrenalin in the locals will increase the time but unless the toothpuller is a tortoise it’s really not needed.
Change your dentist.
One of the main effects of getting older is that the elasticity of the arterial vessels reduces, as they become stiffer (and probably, calcified, in most westerners particularly). This means that their elastic recoil isn’t as able to absorb the sudden increase in arterial pressure that comes with systole.
Also, organs will start, over time, to adjust their autoregulation abilities, so they become accustomed to running with higher blood pressures, and will then misbehave when the pressure drops.
Congrats on being the one person in a thousand willing to take medical advice and look after themselves. Everyone else just wants a pill, and to take no personal responsibility for their health, especially if they have to give up anything they like. (I’m in the 999 myself, but hopefully one day I’ll change (though probably too late).)
White coat syndrome is a real phenomena too, perhaps as high as 1/3 of patients. Just getting your blood pressure taken in a doctor’s office makes it high enough to result in a misdiagnosis. Conversely home based monitoring can trigger hypochondria. Then there is the direct impact of pain on BP results. Actually getting good well normalised data for BP over time takes more than accurate technology.
There is an additional way it can be done in critical care departments and is hinted at in the text above. ‘Invasive’ monitoring – where a plastic cannula tube is inserted into an artery (wrist, elbow, groin, usually), and attached to a pressurised bag of fliud and a transducer. The transducer is zero’d at atmospheric pressure, and will then record the peak (systolic) and trough (diastolic) pressures on a beat-to-beat basis. It’ll also give you a continuous waveform of the pressure changes with each heartbeat.
It has a couple of other advantages – being beat to beat, it’ll react immediately if there’s a problem, and also you can infer several things (about myocardial contractility and vascular resistance) based on the waveform itself.
There is no requirement for testing and calibration of these in doctor’s offices, in Canada at least.
The tubing and cuff can leak, sensor shift etc. They don’t last forever.
Caused me great trouble because my GP’s reads at least 30mmHg low. Found out the hard way at other clinics freaking about hypertension. The company making the (really good actually) product went out of business almost 10 years ago. So GP’s got old units.
At home, the Omrons are terribly inconsistent, but they blame it on your body. Not the crappy tech Omron has. Never the same reading, drives me nuts. Am I dying or not.
This has been said, but is worth repeating: If you don’t consistently sit quietly and relax for five minutes, the readings will likely trend high, probably by quite a bit more than any inaccuracy of a halfway decent instrument.
Maxim makes an optical chip that can take BP. Not (not!) easy to program. But it does a pretty good job on at least some skin types. You need to have a bone behind the skin for reasonable readings (wrist, forehead).
I put it into a device about 4-5 years ago. It really does work.
I worked for a company who made, amongst other devices, a blood pressure measurement device. It was of the inflatable cuff type, and had quite a good dsp and algorithms inside to do the work, not like the cheap $30 devices. The device underwent clinical trials and the measurements were very good, corresponding quite good to what the doctor would read when doing a manual blood pressure measurement. Of course, provided that the patient would keep to the instructions. All very interesting work.
Sadly, the company went bankrupt because of some short seller investment group targeted our company’s main investor, and our main investor pulled out their investments because they got into a whole lot of trouble and got cold feet. The short seller made a few million dollars, and at least 5 startup healthcare companies went bankrupt. And people wonder why healthcare is unaffordable…
Anyway. It would have been nice to use Milos’ knowledge to see how close we were to the ideal, and if we could get any closer.
I think the electronic devices are infinitely better than taking the reading manually, for 1 reason. They use documented algorithm and do it the same way every time. I’ve watched nurses take me and my wifes blood pressures many times, and despite the seriousness of it, they almost always half ass it. They throw that cuff on over clothing, don’t bother with body positioning, and they drop the pressure in only a few seconds. If her heart is beating at 60bpm, how many mmHg is the needed dropping between heartbeats? Quite a few. I’m sure it’s possible to get an excellent reading manually, but I don’t think I’ve ever seen a nurse attempt it.
I love how complex terms like:
systolic pressure and diastolic pressure
are used in medicine. The big number (systolic) is the maximum pressure (in mm of mercury ; ~16 kilopascalsl ;~2.3 PSI) inside your arteries as your heart pumps out blood (while resting). And the smaller number is the pressure inside your arteries between the beats of your heart (~10 kilopascals ; ~1.5 PSI).
They are basically a measurement of how hard your heart has to work while idle. If your arteries are coated with a layer of fat the amount of work that your heart needs to do increases.
You say fat, and yet the compounds often said to cause high blood pressure are not fat.
Seems it’s a bit more complex.